Step 3. Conducting health planning using a co-design process
Conducting the co-design process
This step outlines how the co-design process was implemented through the project. It is presented in three sections:
- content for each step in the co-design process
- facilitating participation
- tips for implementation.
Content for each step in the co-design process
The co-design process utilised in our project involved four steps. Each step was carried out via workshops, small group or individual meetings. Co-design workshops and interviews were held in person in each community and online. The four steps in the co-design process are summarised in Figure 4.3.1.
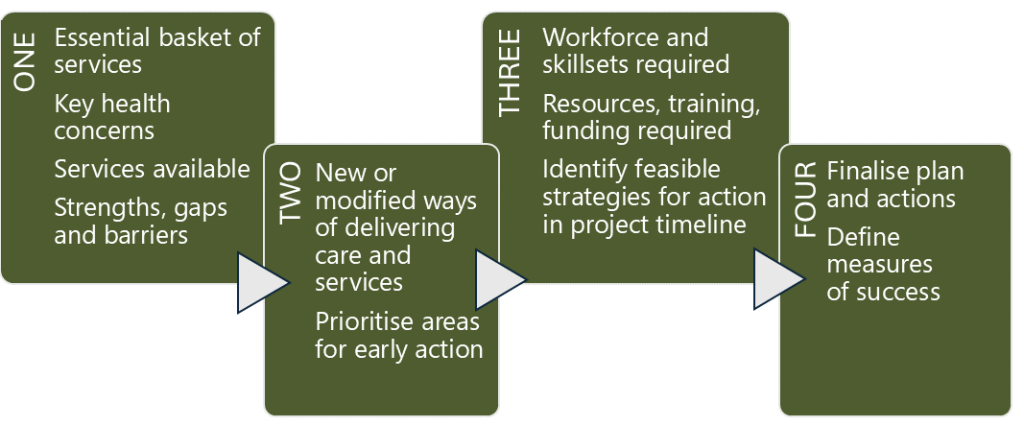
Workshops ran for approximately two hours each, with refreshments provided. Although the team began each session with defined objectives, flexibility was necessary to adapt the workshop plans and follow the flow of discussions as they unfolded naturally. The objectives for each step were as follows:
Step 1: Community and Service Mapping
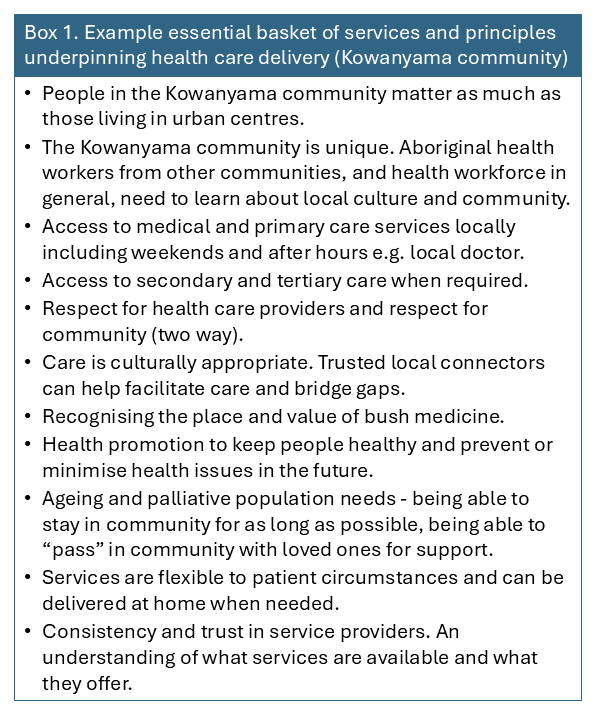
- to confirm essential basket of services and principles that underpin health care delivery (see Box 1 for an example from the Kowanyama community)
- explore the local population and their characteristics
- identify environmental, social or cultural issues affecting health
- to confirm current services available (current model of service delivery)
- to identify strengths, gaps and barriers.
Step 2: Exploring key priorities and models of care
- to discuss gaps and barriers
- to explore new or modified models of health care delivery
- to prioritise areas for early action.
Step 3: Identifying resourcing needs and strategies
- to discuss the prioritised actions to determine workforce and skillsets required
- to determine resources/training/funding required to implement actions
- to identify feasible strategies for inclusion in project.
Step 4: Confirming an action plan and evaluation framework
- to confirm the action plan for the project, including the responsible party and timeframes
- to define measures of success.
At the end of each step, all discussions were compiled and summarised in detailed reports. These summaries serve as a vital record of conversations and decisions, and they help keep those who couldn’t attend updated on progress. It is important that these summaries be shared with all participants for review to validate their accuracy.
Progress updates should also be communicated to the wider community to ensure everyone stays informed and engaged. Use a variety of communication channels to reach different audiences effectively. After each step, articles were published in local newsletters and newspapers. Social media proved effective in some communities, though less so in others. For individuals without internet or social media access, consider distributing printed copies directly. In areas where literacy or language may be a barrier, providing translated or simplified materials is recommended.

Appendix 6 – Questions for workshops: outlines question sets that were developed to guide the implementation of each workshop to explore the objectives and help guide discussions. These may be used or adapted to support planning work. While the approach undertaken in this project was broad, questions may be adapted to focus on a particular topic or population group within the community.
Appendix 7 – Workshop session plans: presents session plans for each workshop, including timeframes and resources required. The plans were developed to take a broad approach and may be used or adapted to suit.
All summaries from the project are available on the project website: https://www.taahc.org.au/research/integrating-health-care-planning-for-health-and-prosperity-in-north-queensland/project-communities/

Listen to our Local Connectors talk about how the co-design process worked in their communities:
A note on prioritisation
Prioritisation may take place at various points throughout the process. In steps one and two of the place-based planning project, in all three communities, there were many areas for improvement identified, and within each area, many actions were proposed. Early prioritisation can be undertaken at the end of step two to narrow down areas on which to focus.
One simple approach to facilitate early prioritisation is asking all participants to list their top three areas for improvement (anonymously), and collating results to identify the top three areas. These results are then presented back to all participants for validation.
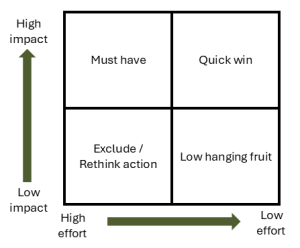
Drilling down into these priority areas, each action can then be further assessed according to a prioritisation matrix (see Figure 4.3.2), to identify those that are most or least important (will have a high or low impact) and the level of resourcing that will be required (will need high or low effort). A way of facilitating this assessment of feasibility is by presenting the list of actions on a chart, and inviting participants to put a dot against each action, to indicate in which of the four squares they believe the action sits (Figure 4.3.3). Depending on the timeframe in which to complete the planning work and conduct implementation, this method could be applied to all actions.

Collaboratively examine the prioritised actions to assess their feasibility for implementation, taking into account their importance and the resources required, such as funding, materials, human capacity, training, and timeframes. It is also important to identify complex intersectoral priorities, understand where decision-making power lies, and explore the necessary steps to achieve the desired outcomes.
Some actions may be identified as “quick-wins” or “low-hanging fruit” innovations that are simple to execute and have low and high impacts. Other actions may be complex and high-impact innovations that might take longer to execute or may be resource-intensive. Some actions may demand significant effort but result in minimal impact, and therefore may be set aside or excluded.
Facilitating participation
The local reference group and local connector are best placed to advise on how to continue to engage with community stakeholders and encourage participation throughout the co-design process and implementation phase.
Provide a variety of options for engagement. Offer a few time slots for face-to-face participation. Evening workshops may be more suitable for the working community, and morning workshops for families and older adults. Consider lunchtime workshops for health and community service providers. If understanding language is a concern, consider the use of interpreters.
Consider social and structural factors, for example, cultural safety, community dynamics and accessibility, that may affect the ability of stakeholders to attend engagement activities. Consider how stakeholders can be supported in participating. For example, can project funding be used to support accessibility with transport?
Consider the stakeholders that may attend and how the dynamics of engagement activities may be affected. Build in appropriate engagement opportunities to support inclusion and accept that other priorities may crop up for stakeholders, necessitating other mechanisms for engagement.
The option to participate via online workshops is a useful supplement to in-person engagement and supports an inclusive approach. Build in alternatives to gatherings of individuals as the primary strategy for engagement. Provide the option for separate meetings, written input or oral inputs with translation. Take the workshop or activities to the participants and deliver in a space where they are comfortable, or link in with existing meetings or gatherings of local groups.
Maintain open communication channels by ensuring that contact details are available, particularly those of the local connector and/or partner organisation workers.
Recognise expertise and participation by community members through appropriate catering, travel support and/or financial reimbursement.
Conducting the co-design process
Within the place-based planning project, the full co-design process was fully implemented in both Hughenden and Clermont. In both communities the four rounds of co-design workshops were conducted over six months, with each round held approximately every two to six weeks apart depending on availability of participants and working around planned and unexpected events.
In the project there were no funds available for implementation. This made the assessment of feasibility and prioritisation of actions very important. Assessing impact and effort, including any requirements for human resources, materials or funding, was critical to identify cost-neutral actions that could be implemented during the project timeframe.
The place-based health plans provided evidence of community need. The plans could be used as evidence to advocate for further funding or resources beyond the project in pursuit of longer term or resource intensive actions.
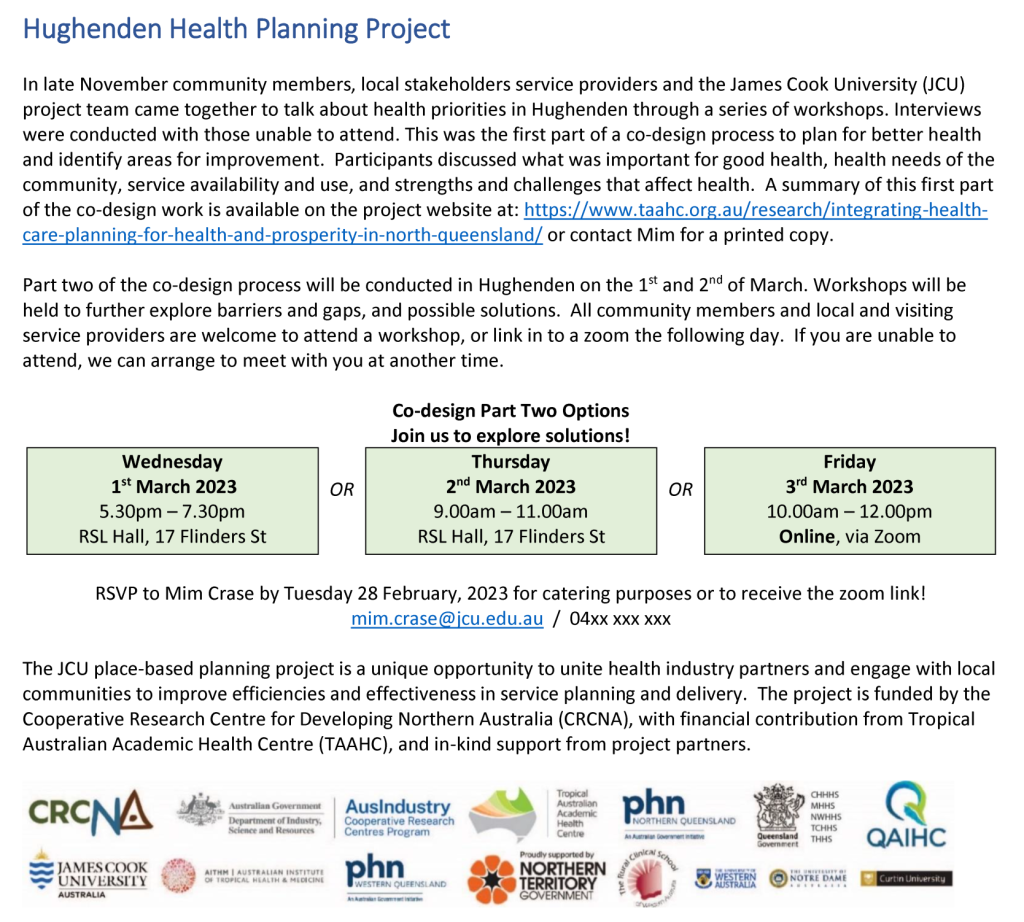
Example of an update for community and advertising the next round of workshops
It’s important to share progress updates with the broader community to keep everyone informed and involved. Local newsletters and social media were key communication methods used within the communities. An example is provided in Figure 4.3.4.
Tips for the implementation of co-design activities
Consider workshop availability and accessibility in terms of location and timing:

- our team used easily accessible and common gathering places, including community halls and local cafes (see Figure 4.3.5)
- workshops for each step were run in-person twice, once after hours and once during working hours
- refreshments were always provided. Transport was able to be provided on some occasions
- a workshop was also offered virtually for those unable to attend.
Consider a series of separate meetings for those unwilling or unable to attend workshops:
- when key stakeholders did not attend, separate meetings were arranged to ensure that pertinent views and diverse opinions were incorporated
- produce accessible summaries for each step of the process and disseminate them to all active participants and interested passive participants
- brief updates in newsletters were a great option to reach the broader community.
In co-design activities, encourage participants to think creatively and aspirationally, but aim for cost neutrality:
- creative thinking, aspiring to optimal health and health care delivery is welcomed, and should initially not be constrained by funding, policy or service delivery silos
- in terms of prioritising actions, starting with the principle of cost neutrality – i.e. redeploying existing funds and resources – is often most successful.
Obtain feedback immediately following participation in co-design activities to inform improvements for subsequent engagement and collaboration.
- anonymous surveys are a quick and effective tool.
Appendix 8 – Evaluation survey: provides an example of a simple workshop evaluation survey.
Listen to our Clermont Local Connector talk about benefits for participants:

Encourage broad participation in co-design activities to discuss strengths and challenges, identify community needs, explore potential solutions, and prioritise feasible actions. Localised approaches will help uncover solutions that are relevant and responsive to the specific context.
