2.11 Beta-Adrenoceptor Antagonists
John Smithson
Beta-Adrenoceptor Antagonists (aka Beta-blockers)
In this topic we will further explore the sympathetic nervous system looking at drugs that affect the cardiovascular response. This chapter will focus on Beta-adrenoceptor antagonists also known as Beta-blockers.
Learning Outcomes
Be able to:
- Understand how Beta Blockers exert their effect at a cellular level
- Understand the mechanism by which the heart muscle contracts and how Beta Blockers decrease contractility
- Understand how Beta Blockers are classified and how this impacts on their activity
- Recognise the main Beta Blocker drugs and their most common adverse effects.
Beta-adrenoreceptor antagonists
Beta-adrenoreceptor antagonists or beta-blockers competitively block the effect of catecholamines (noradrenaline and adrenaline) at the beta-adrenoceptors. While beta receptors are widely distributed throughout the body, beta2 receptors are found mainly in the smooth muscle of the airways and beta1 receptors are located in large populations in myocardial tissue. When the sympathetic nervous system releases noradrenaline or adrenaline, the beta-antagonist blocks the effect of the catecholamine thus reducing heart rate and contractility associated with beta receptor stimulation.
How does the beta antagonist work at a cellular level?
The beta1 receptor is a Gs-coupled protein receptor as seen below in the figure below.
The binding or noradrenaline (or adrenaline) to the beta1 receptor on the cardiac myocyte under normal conditions activates adenylyl cyclase which promotes the conversion of ATP to cAMP. Increased levels of cAMP activates cAMP-dependent protein kinase (PK-A). PK-A opens L-type calcium channels increasing the amount of calcium (Ca2+) in the cardiac monocyte as well as encouraging the release of calcium from the sarcoplasmic reticulum. The increased intracellular calcium binds to cardiac troponin-C component of the troponin complex on the actin thin filaments on the cardiac muscle.
This moves tropomyosin out of the way allowing the myosin head to interact with the actin facilitating contraction. In short, increased intracellular calcium allows more myosin heads to interact with the actin filament on the cardiac muscle – this allows an increased contraction of the muscle tissue (see video explanation below).
Beta-antagonists block the action of the catecholamines at the beta-receptor thereby decreasing the amount of intracellular calcium that is available and this in turn reduces contraction of the heart.
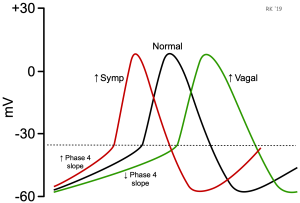
The effect of the beta-receptor on heart rate is also linked to intracellular calcium stores. Stimulation of the beta-receptors in the SA node, AV node and atrial tissue increase the intracellular concentration of calcium in a similar fashion to that described previously – it facilitates the opening of L-type calcium channels allowing the movement of calcium into the cell and encourages the release of calcium from the sarcoplasmic reticulum. The increase in intracellular calcium levels alters the electrical potential of the cell bringing it closer to threshold (about -40 to -30 mV) where phase 0 of the action potential (depolarization) can occur (see figure below).
📺 Watch: For a video explanation of how calcium increases contraction of the cardiac myocyte:
There are three main groups of the beta-adrenoreceptor antagonists:
- B1-selective blockers or cardioselective blockers because they block Beta1-adrenoceptors mainly located in the heart.
- Non-selective B-adrenoreceptor antagonists which block both types of adrenoreceptors B1 and B2, and
- Non-selective B-adrenoreceptor antagonists with intrinsic sympathomimetic activity (ISA) which causes partial stimulation of the B-adrenoreceptor with the effect being less than that of a pure agonist.
The blockade of B1 receptors in myocardial tissues produces the following effects:
- In the Sinoatrial node blockade reduces heart rate (negative chronotropic effect)
- In the Myocardial tissue blockade reduces contractility (negative ionotropic effect)
- In the Juxtaglomerular cells in the kidney blockade reduces the release of renin (important in the reabsorption of sodium in the distal tubule and collecting ducts)
- In the Central nervous system blockade reduce outflow of the sympathetic nervous system from the medulla oblongata.
The reduction in heart rate and contractility combined with a reduction in the release of renin and a reduced outflow of the sympathetic nervous system reduces blood pressure – a very common use of beta-blockers.
The effect of beta-blockers on a resting heart is modest, it exerts a more significant reduction in heart rate and contractility during exercise, so beta-blockers also reduce exercise tolerance. The benefit of a reduction in heart rate and contractility aside from a reduction in blood pressure is it also reduces myocardial tissue oxygen demand, which makes it useful in people with conditions with reduced coronary artery blood flow (for example angina).
Listed below are the B-adrenoreceptor antagonist (Beta Blocker) drugs in their classifications:
Beta-blockers can also be classed according to their lipid solubility. The lipid soluble beta-blockers tend to have greater central nervous system adverse effects (they penetrate the CNS more readily) and are typically metabolized by the liver. Most beta-blockers are lipid soluble. Where unwanted central nervous system side effects occur with the use of beta-blockers, for example, nightmares, a beta-blocker with low lipid solubility such as atenolol or sotalol may be more appropriate.
Common adverse effects of beta blockers
There are some clinical conditions where beta blockers are contraindicated because of their adverse effects such as in asthma and chronic obstructive pulmonary disease (COPD). This is because Beta blockers can precipitate bronchospasm leading to airway compromise. Remember that the B2 receptor was found on the smooth muscle of the airways?
Other adverse effects include bradycardia, orthostatic hypotension, cold extremities, fatigue, changes in glucose and lipid metabolism and they can have a transient negative effect on symptoms of heart failure.
Read section 6.3.6 Beta-blockers (Page 277-282) in Australian Medicines Handbook. Adelaide: Australian Medicines Handbook Pty Ltd; 2020
📺 Watch: The recorded video on beta-blockers. (31:36 min)
Summary
- Selective beta blockers affect mainly Beta1 receptors in the myocardial tissue.
- Non-selective beta-blockers interact with Beta1 receptors and Beta2 receptors accounting for some of the respiratory side effects
- Beta-blockers can be stratified by beta-selectivity, lipid solubility and intrinsic sympathomimetic activity
- Beta-blockers block a G-protein coupled receptor which ultimately reduces calcium in the cell reducing automaticity (slowing heart rate) and decreasing contractility.
- Beta-blockers have a modest effect at rest – they have a more significant effect during exertion.
COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING
This material has been reproduced and communicated to you by or on behalf of James Cook University in accordance with section 113P of the Copyright Act 1969 (Act).
The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice.