Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
6.1.3 Chronic Complications of Diabetes (Microvascular and Macrovascular)
Learning Outcomes
Be able to:
Describe the complications of poorly controlled diabetes
Describe the implications of and screen patients for diabetes risk and refer appropriately
Apply symptoms and pathology to the diagnosis of diabetes
Apply knowledge of the management of T2DM to patients with uncomplicated disease
Apply knowledge of the management of T1DM to patients with uncomplicated disease.
Why do high BGLs matter?
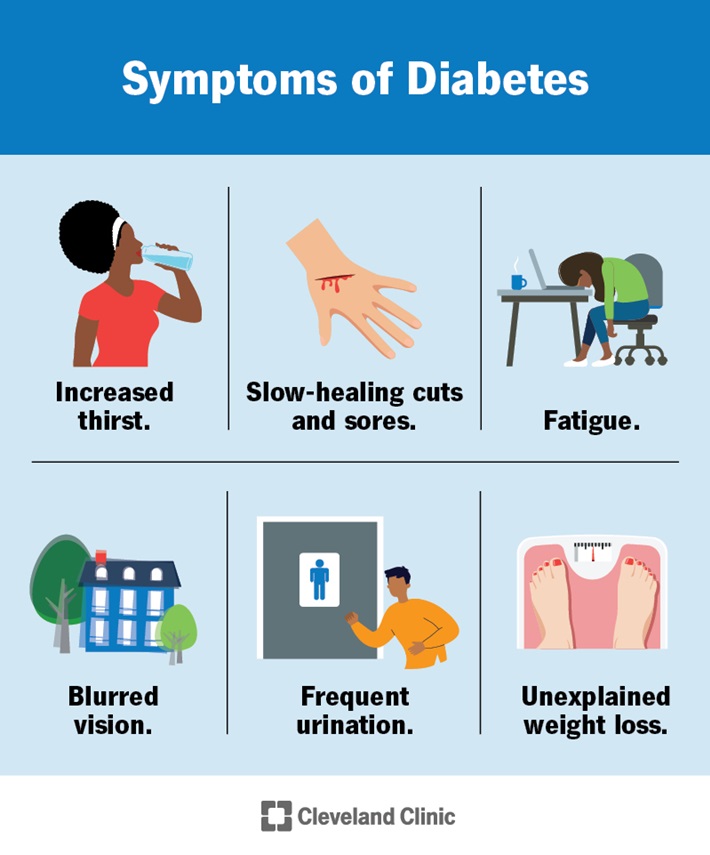
When we consider the impact of diabetes, we need to consider both the short and long-term consequences. In the previous section we already discussed two particularly important acute complications of hyperglycaemia, including DKA and HHS. Both DKA and HHS are medical emergencies and present with dehydration and electrolyte abnormalities in addition to BGL elevations (normally). The dehydration and electrolyte abnormalities are usually secondary to renal losses associated with polyuria and nausea/vomiting limiting intake. Thinking back to diuretics from week 2, you can see how elevated BGLs lead to an osmotic diuresis. The classic symptoms of elevated BGLs that can occur with both T1DM and T2DM include:
Source: Diabetes: What It Is, Causes, Symptoms, Treatment & Types (clevelandclinic.org)
Elevated BGLs are also associated with:
Direct glucose mediated endothelial damage
Oxidative stress
Advanced glycation end products
Inflammation and inappropriate growth factor production
What does sustained hyperglyaemia lead to?
These processes lead to many of the significant vascular, renal and ophthalmic complications of poorly controlled diabetes. You don’t need to understand the images below in detail but they provide a nice overview of mechanisms of glucose mediated damage in different organs.
Image sequence – click to slide across
Much emphasis is placed on reducing the microvascular and macrovascular complications of diabetes and the associated morbidity and mortality.
Microvascular complications include:
Diabetic kidney disease
Diabetic retinopathy
Diabetic neuropathy
Macrovascular complications include:
Ischaemic heart disease
Cerebrovascular disease
Peripheral vascular (arterial) disease.
“But I feel fine”
Many patients with T2D may be relatively asymptomatic. For an asymptomatic patient, we are usually most concerned with reducing their risk of developing chronic complications of diabetes. Pharmacotherapy plays an important role in achieving this goal in conjunction with non-pharmacological measures. When diabetic complications are considered, diabetes is estimated to contribute to around 21,900 deaths per annum in Australia (approximately 11% of all deaths). The objectives of diabetes management include:
Optimise quality of life
Relieve symptoms of hyperglycaemia
Avoid acute complications of hyperglycaemia, such as diabetic ketoacidosis and hyperosmolar hyperglycaemia
Avoid hypoglycaemia
Reduce chronic complications of hyperglycaemia.
Source: 2023 Snapshot: Diabetes in Australia – Diabetes Australia
📺Watch this video on the chronic (micro- and macrovascular) complications of sustained hyperglycaemia in diabetes.
Download the lecture notes here:
Check Your Understanding:
COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING
This material has been reproduced and communicated to you by or on behalf of James Cook University in accordance with section 113P of the Copyright Act 1969 (Act).
The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice.