4.2.3 Chronic Kidney Disease
Learning Outcomes
Be able to:
- Explain the aetiology & pathophysiology of CKD
- Describe the approach to diagnosis and staging of CKD
- Describe the pathophysiology of common complications of CKD
- Explain how complications of CKD are managed with medications.
Chronic Kidney Disease
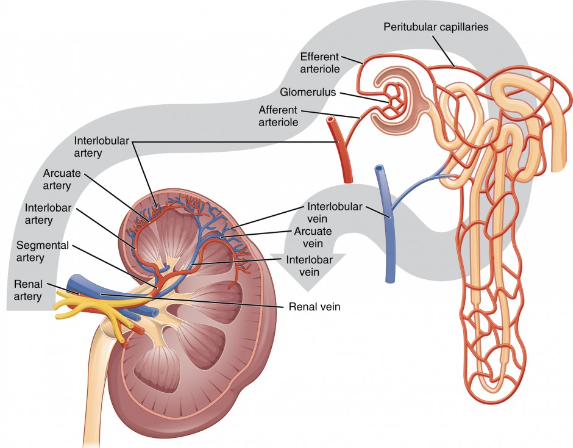 |
 |
 |
Chronic kidney disease is defined as:
- An estimated or measured glomerular filtration rate (GFR) < 60ml/min/1.73m2 that persists for ≥ 3 months and/or
- Evidence of kidney damage that persists for ≥ 3months, evidenced by either:
- Albuminuria
- Haematuria (after exclusion of urological causes)
- Structural abnormalities (e.g., identified by medical imaging)
- Pathological abnormalities (e.g., identified by renal biopsy)
CKD is highly prevalent worldwide, affecting approximately 9-13% of adults. In Australia, we know that the prevalence is about the same as it is internationally, with approximately 10% of Australian adults meeting the diagnostic criteria for CKD.
Unfortunately, considerably higher rates of CKD are found in:
- Aboriginal and Torres Strait Islander people
- People living in remove areas
- People living in areas of socioeconomic disadvantage
This geographic and demographic spread is important to understand for the purposes of both primary prevention and management of CKD.
What’s also important to understand is that CKD often goes undiagnosed until it has progressed to its most advanced stages. This is explained largely by the fact that CKD is commonly asymptomatic. Up to 90% of kidney function may be lost before symptoms attributable to the accumulation of toxins and excess fluid present. Such symptoms include pruritis, nausea, vomiting, lethargy, and dyspnoea, to name just a few.
The most common causes of CKD are sub-optimally controlled diabetes and hypertension. So, glycaemic control and optimisation of blood pressure are essential for slowing the progression of chronic kidney disease. Other risk factors include established cardiovascular disease, a family history of kidney disease, obesity, smoking, age greater than 60 years, and history of acute kidney injury.
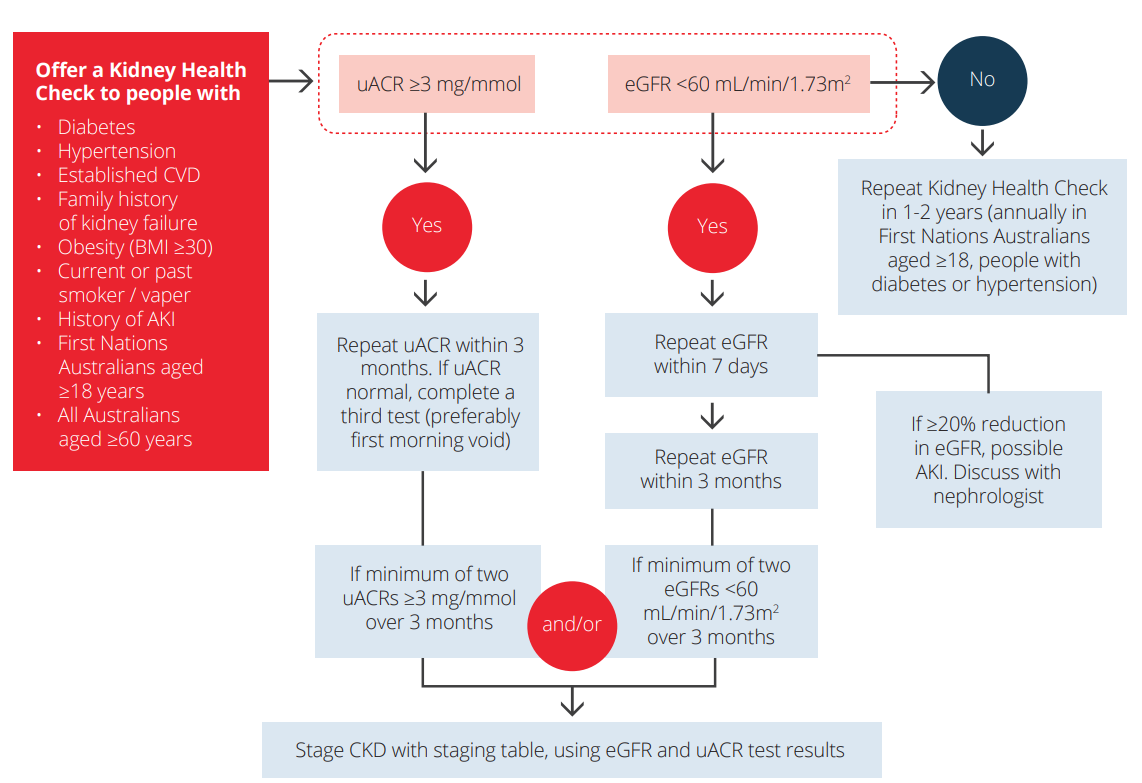
Regular screening for CKD (every 1-2 years) is recommended for people with risk factors for CKD. This regular screening will include:
- A blood test, that is specifically looking at serum creatinine levels and the eGFR
- A urine test, to determine if there is any albumin present in the urine and report the urine albumin:creatinine ratio (urine ACR)
- A blood pressure test to identify and manage hypertension
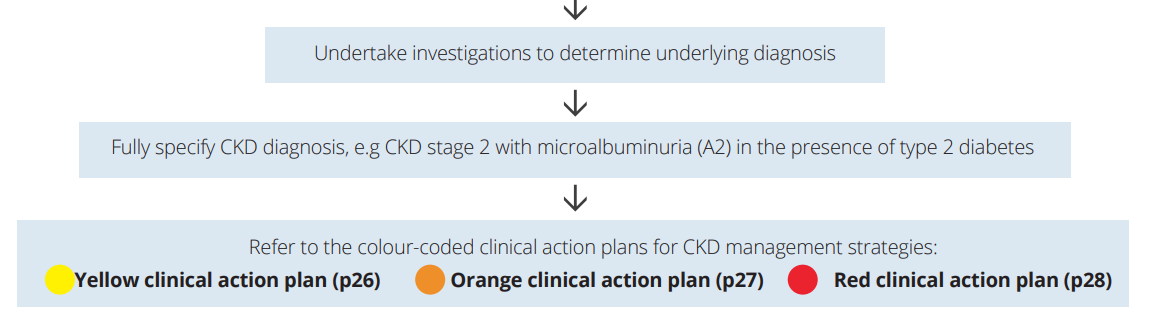
The results of the blood and urine test screening will be interpreted using this flow diagram, which also informs time frames for follow up / repeat measurements if the initial result is normal or abnormal.
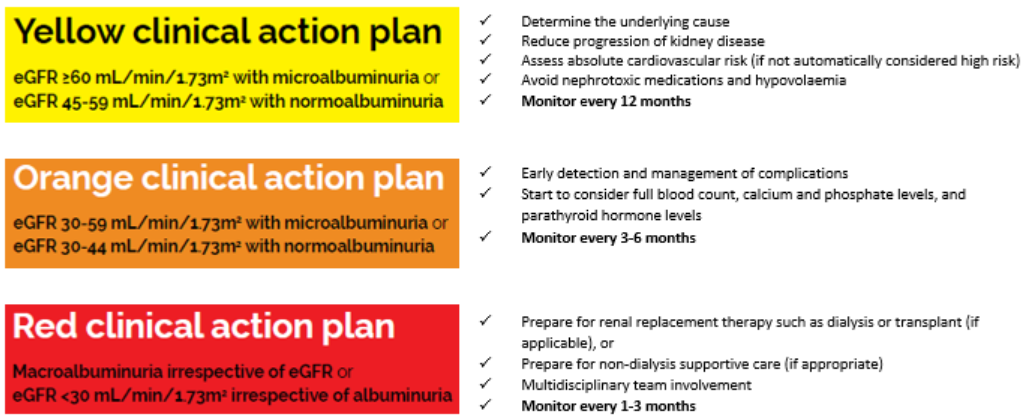
Once the diagnosis of CKD is made, then the severity of the CKD is staged based on both the eGFR and urine ACR. The colours on the staging chart below are used to differentiate different approaches to the treatment of CKD, depending on its severity.
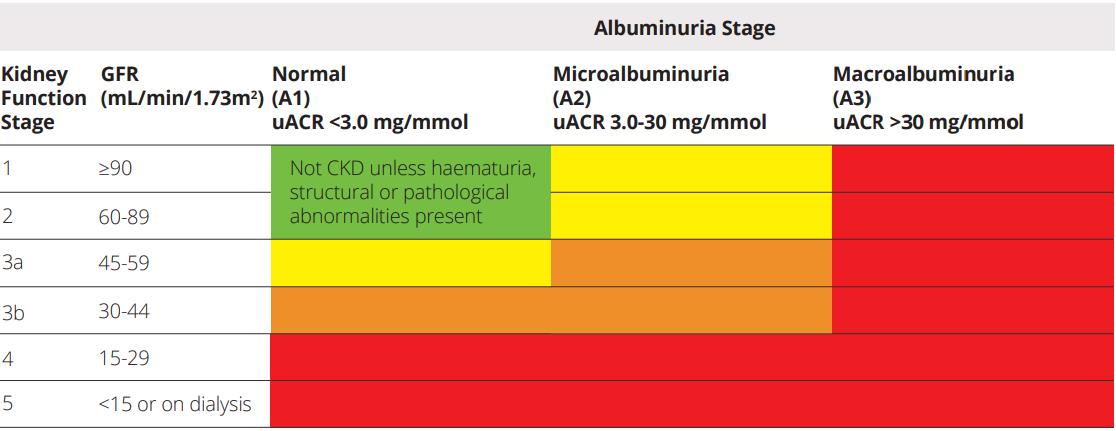
However, it is also important to remember that CKD itself is not a diagnosis. There is a need to identify the underlying cause to complete the diagnosis and decide on the most appropriate treatment pathway.
📺Watch this video on Chronic Kidney Disease (22:33 minutes)
There are a variety of different complications of chronic kidney disease, including:
- Hypertension (often a pre-existing condition)
- Albuminuria
- Acidosis
- Anaemia
- Hyperkalaemia
- Hyperphosphatemia
- Hypocalcaemia
- Hyperparathyroidism
- Oedema
- Pruritis
- Restless legs
- Uraemia
📺Watch this video on complications of Chronic Kidney Disease (48:37 minutes)
📚 Read/Explore
- Read Kidney Health Australia. Chronic Kidney Disease Management Handbook (5th Ed). Kidney Health Australia webpage. Updated in 2024. Available at: https://kidney.org.au/health-professionals/ckd-management-handbook. KHA-CKD-Handbook-5th-Ed-July2024
- Read the article below regarding when and how drug doses should be adjusted in chronic kidney disease. How to Adjust Drug Doses in Chronic Kidney Disease
- You may find it useful to complete the following table to help you learn this material.
-
Pathophysiology Treatment Hypertension Albuminuria Acidosis Anaemia Hyperkalaemia Hyperphosphatemia Hypocalcaemia Hyperthyroidism Pruritis Oedema Restless legs Uraemia
-
- Read the following patient information brochure that aims to empower Aboriginal & Torres Strait Islander people to improve their kidney health. Kidney Health Australia Flipchart
- Explore the following patient information brochure that aims to help patients with diagnosed CKD make informed decisions about their treatment. Kidney Health Australia Resource to Aid Patient Decision Making