2.1.4 Diuretic Pharmacology
Learning Outcomes
Be able to:
- List the different types of diuretics and their uses in the clinical setting
- Explain the mechanism of action for each type of diuretic
- Describe common side effects and the implications for patients taking these drugs.
Revision of Anatomy and Physiology of the Renal System
 |
 |
 |
An understanding of renal anatomy and physiology is critical to your understanding of the action of drugs that affect the renal system such as diuretics. You are already familiar with this system but as you progress through this week’s work, you may want to refer back to the following sections to ensure you have a good understanding. The most important renal system anatomical and physiological concepts you may want to revise from your anatomy and physiology text [Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019] are:
- Blood and nerve supply of the kidneys (Page 1459–1461 of above text)
- The nephron (Page 1461-1467 of above text)
- Glomerular Filtration Rate (P1470-1473 of above text)
- Renal autoregulation of GFR.
- Neural regulation of GFR.
- Hormonal regulation of GFR.
- Principles of tubular reabsorption and secretion. (Page 1473-1476 of above text)
- Reabsorption and secretion in the proximal convoluted tubule. (Page 1476-1479 of above text)
- Reabsorption in the nephron loop. (Page 1479-1481
- Reabsorption in the early distal convoluted tubule. (Page 1481 of above text)
- Reabsorption and secretion in the late distal convoluted tubule and collecting duct. (Page1481 of above text)
- Homeostatic regulation of tubular reabsorption and tubular secretion. (Page 1481-1485 of above text)
- Production of dilute and concentrated urine. (Page 1485-1491 of above text)
Introduction to Diuretics
|
|
|
There are four main classes of diuretics:
- Loop diuretics such as frusemide, bumetanide and etacrynic acid.
- Thiazide diuretics such as hydrochlorothiazide and indapamide
- Potassium-sparing diuretics such as amiloride and spironolactone and lastly
- Osmotic diuretics such as mannitol.
Of the four types, osmotic diuretics such as mannitol are the most potent and one of the least commonly used. The two most commonly used diuretic classes in Australia are loop diuretics (i.e. frusemide) and thiazide diuretics (hydroclorothiazide). Diuretics are used for hypertension and a broad range of conditions that require fluid load reduction such as cirrhosis, partial renal failure and oedema, symptomatic management of congestive heart failure and other conditions that result in peripheral oedema.
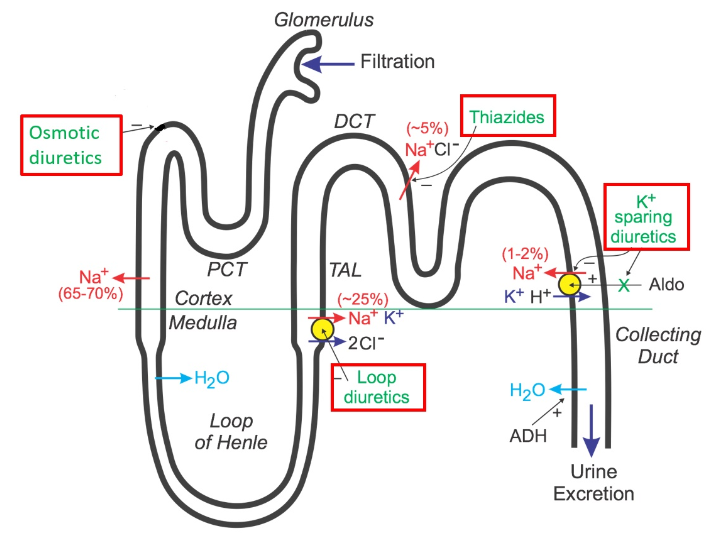
All diuretics modify renal function to reduce the reabsorption of water from the filtrate via the common mechanism of increasing sodium excretion in the filtrate.
📺 Watch the video on an Introduction to Diuretics (9:33 minutes)
Loop Diuretics
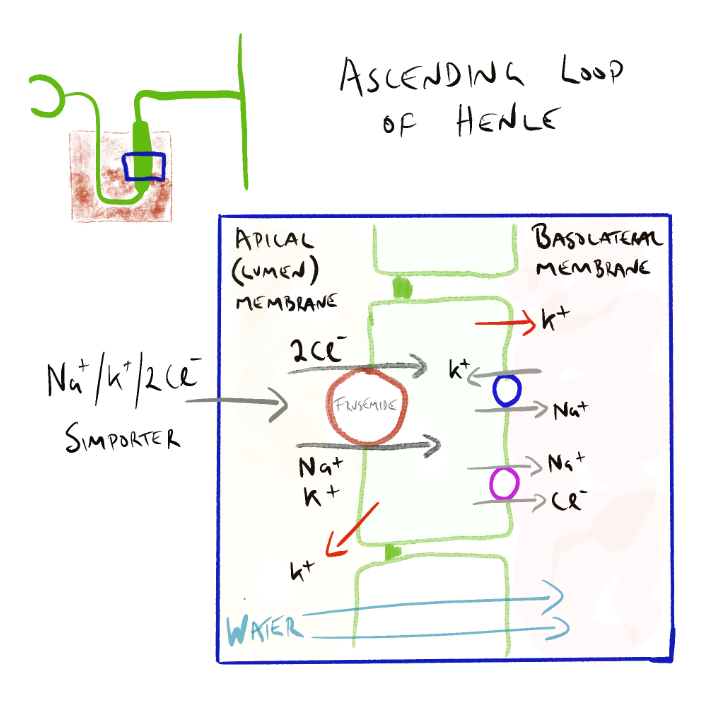
Of the 3 available loop diuretics frusemide, bumetanide and etacrynic acid – frusemide is the most commonly used agent. Loop diuretics are a moderately potent diuretic second only to osmotic diuretics. They are all relatively short acting lasting about 4-6 hours. Their potency results from their site of action on the nephron – that site being the thick ascending loop of Henle. Loop diuretics are used for conditions that require fluid load reduction but unlike thiazide diuretics are not used in the management of hypertension.
Loop diuretics are actively secreted into the lumen via the proximal tubule. In the Loop of Henle, they inhibit the Na+/K+/2Cl– cotransporter reducing sodium reabsorption (see figure below). As water follows sodium, the increased sodium concentration in the filtrate reduces the osmotic gradient reducing water movement back into the interstitial space surrounding the nephron (and eventually the blood). Loop diuretics are so potent because the Loop of Henle is the major site of sodium reabsorption – accounting for between 15-25% of sodium and chloride reabsorption normally.
Side Effects of Loop Diuretics
Frusemide and other loop diuretics can cause electrolyte disturbances (calcium, potassium, sodium, chloride, magnesium loss) though this is dose related. Other common side effects include postural hypotension, dehydration, dizziness, rash and metabolic alkalosis (H+ is lost in the filtrate also due to loop diuretic effect). They can also precipitate gout (they decrease excretion of uric acid) and cause ototoxicity. Ototoxicity is uncommon in normal doses but can occur when administered with other ototoxic drugs. On their own, loop diuretics typically only cause temporary hearing loss. Rarely, permanent deafness can occur when diuretics are used in acute or chronic renal failure or in combination with other ototoxic drugs such as aminoglycosides, cisplatin, carboplatin and NSAIDS.
Unlike other diuretics, loop diuretics are high-ceiling diuretics. This means they are effective over a very broad range of doses and the greater the dose given, the greater the effect. This is useful in renal impairment. However like all drugs, the higher the dose, the higher the risk of side effects – particularly sodium and potassium loss and ototoxicity.
📺 Watch the video on an overview of Loop Diuretics (5:18 minutes)
📚 Read/Explore
- Read Loop diuretics in Chapter 30 The kidney and urinary system (page 389-399) in the 9th edition Rang and Dale’s Pharmacology.
Thiazide Diuretics
Thiazide diuretics are commonly used to induce diuresis and as an adjunct therapy for hypertension. Examples of thiazide diuretics include:
- Chlorthialidone
- indapamide
- hydrochlorothiazide.
Like loop diuretics, thiazide diuretics are actively secreted into the filtrate via the proximal tubule. They are transported to the distal convoluted tubule in the filtrate where they block the action of the Na+ /Cl-symporter, reducing sodium and chloride reabsorption. Because the distal convoluted tubule is only responsible for about 5% of the sodium reabsorption, they are much less potent compared with loop diuretics. The sodium concentration of the filtrate is elevated when it arrives in the collecting duct. Here, sodium is transported back into the cells of the collecting duct in exchange for potassium which is transported from the blood to the filtrate (urine). This explains the loss of potassium with thiazide diuretics which is unrelated to its action in the distal convoluted tubule. In addition to sodium, chloride and potassium, thiazide diuretics also cause the excretion of magnesium.
📺 Watch the Youtube video on Thiazide diuretics (6:08 minutes)
Thiazide diuretics are low ceiling diuretics. Their effect on diuresis increases with dose up to a maximum ceiling which in the case of hydrochlorothiazide is about 50mg. They have similar side effects to those of loop diuretics: electrolyte disturbances, orthostatic hypotension, dizziness, rash, incontinence, precipitation of gout, blood glucose derangement. The risk of hypokalaemia for thiazide diuretics and loop diuretics is dose related and increased when given with other drugs that cause potassium wasting.
Potassium Sparing Diuretics
Amiloride, triamterene, spironolactone and eplerenone are potassium-sparing diuretics. Due to the location of action, amiloride, triamterene, spironolactone and eplerenone are considered weak diuretics. There are two major mechanisms of potassium sparing diuretics which we will now discuss.
Amiloride and triamterene inhibit sodium reabsorption in the distal tubule by blocking the sodium channels. They block the exchange of sodium and potassium and therefore preserve serum potassium levels. Specifically, amiloride works by blocking the eNa+C (epithelial sodium channel) on the apical membrane of the epithelial cells. The reduced availability of intracellular sodium reduces potassium exchange via the Na+/K+ATPase in the basolateral membrane. This increases sodium and water concentration of the filtrate and reduces potassium loss. The figure below shows the exchange of sodium at the apical membrane and the subsequent impact on potassium loss in the collecting duct.
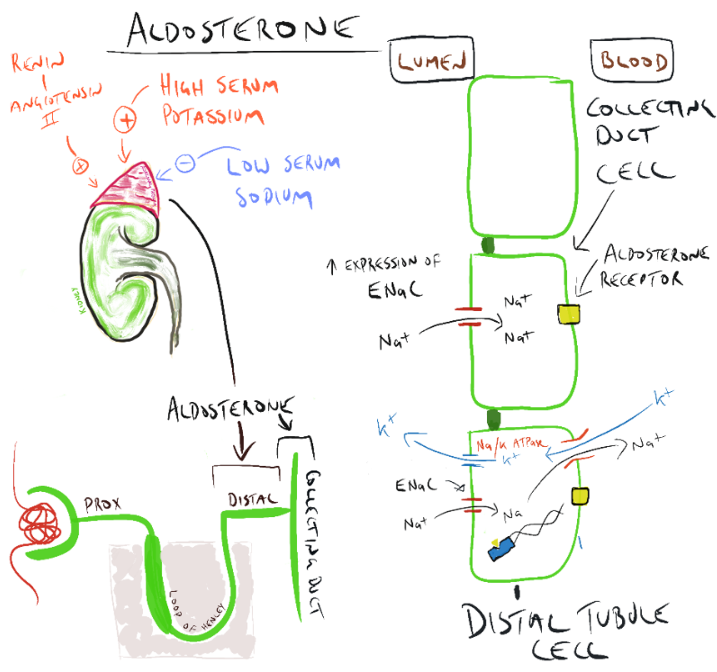
Spironolactone (spirone-o-lac-tone) and eplerenone (ep-ler-e-none) are potassium-sparing diuretics that block the action of aldosterone at the aldosterone receptor in the collecting duct. Aldostrone is released in response to the release of renin and angiotensin II or high serum potassium levels. Aldosterone increases the expression of the eNaC channel on the apical (luminal) membrane and Na+/K+ATPase on the basolateral membrane in the collecting duct. Blockade of the aldosterone receptor by spironolactone or eplerenone reduces water-reabsorbing effects of aldosterone, inhibits sodium reabsorption in the distal tubule and reduce the exchange of sodium and potassium at the basolateral membrane therefore preserve serum potassium levels. Due to the location of action, spironolactone and eplerenone are considered weak diuretics (this section of the nephron is responsible for around 3% of sodium reabsorption.
Side effects of Potassium Sparing Diuretics
Hyperkalaemia is a potential adverse effect especially when combined with potassium supplements or other potassium sparing drugs such as ACE inhibitors and A2RB’s, NSAIDs and trimethoprim. It is prudent to monitor serum potassium concentrations. Other adverse effects include gynaecomastia, menstrual abnormalities and sexual dysfunction with spironolactone.
📺Watch the video on Potassium (K+) Sparing Diuretics (4:09 minutes)
Osmotic Diuretics
Osmotic diuretics such as mannitol are hyperosmotic agents that increase the osmotic concentration of the filtrate, thereby causing significant diuresis. Mannitol is an incredibly potent diuretic due to its site of action – the PCT is responsible for around 65% of sodium reabsorption from the filtrate. It is typically used in the acute management of elevated intraocular, elevated intercranial pressure (ICP) and cerebral oedema (although for the control of elevated ICP and cerebral oedema, hypertonic saline is now more commonly used in ICU).
The most significant effect of mannitol occurs in the proximal convoluted tubule where it increases the osmotic gradient of the filtrate thereby reducing the movement of water from the filtrate to the interstitial space in the kidney which normally occurs under the influence of high sodium concentrations in the interstitial space and the highly permeable nature of the proximal convoluted tubule.
Clinical note: Mannitol is administered by IV infusion when used to reduce elevated ICP. Mannitol crystalises as low temperatures (20 decC), particularly in higher concentrations (mannitol 20% or more). It is important mannitol is agitated or warmed prior to administration to dissolve any mannitol crystals and administered via a large vein through a filter to avoid precipitates being administered.
Side effects and precautions
The adverse effect profile of mannitol is worth noting. Because of it’s powerful osmotic effect both in the nephron but also in the extracellular space, mannitol can:
- precipitate heart failure and pulmonary oedema as it will rapidly increase extracellular fluid volume;
- cause electrolyte imbalances and pH imbalances (acidosis) due to electrolyte and bicarbonate loss in the filtrate;
- cause dehydration and hypotension due to the large fluid volume loss
- confusion and CNS toxicity due to CNS intracellular dehydration, hyponatraemia and acidosis; and
- cause other side effects such as nausea and vomiting, thirst, dehydration, tachycardia, dizziness, hypotension, headache, seizures, hypersensitivity reactions, acute renal failure, fever and angina-like chest pain.
Electrolyte changes
Typically mannitol causes hyponatraemia, hypokalaemia and low levels of other electrolytes. This occurs as the sodium, potassium and other electrolytes are carried out with the filtrate before it can be reabsorbed by the nephron. Conversely, hypernatraemia and hyperkalaemia can occur due to dehydration and haemoconcentration. Blood electrolyte concentrations and renal function should be closely monitored.
📚 Read/Explore
- Revise the renal system and have a good understanding of the different types of diuretics and how they work.
-
- Describe the four types of diuretics and their clinical uses.
- Understand and be able to explain the mechanism of action for thiazide diuretics.
- Describe the pharmacology and side effects of diuretics and what to watch out for in practice.
It may help to put the 4 different types of diuretics in a table to compare/contrast the pharmacology, mechanism of action, side effects and practice points etc. For example:
| Loop Diuretics | Thiazide Diuretics | Potassium-Sparing Diuretics | Osmotic Diuretics | |
|---|---|---|---|---|
| Mechanism of action | ||||
| Site of action | ||||
| Potency | ||||
| Effect on electrolytes | ||||
| Side effects | ||||
| Clinical uses | ||||
| Practice Points |
Download the lecture notes here:
COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING
This material has been reproduced and communicated to you by or on behalf of James Cook University in accordance with section 113P of the Copyright Act 1969 (Act).
The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice.