2.2.1 Dyslipidaemia and Hyperlipidaemia
Learning Outcomes
Be able to:
- Explain the prevalence of raised cholesterol levels in western countries and identify the specific age brackets where prevalence peaks for both men and women.
- Analyze the trends in cholesterol levels in Australia identifying the changes in prevalence and understanding the implications of these trends on public health.
- Interpret age-related data on high cholesterol prevalence, describing the significant increase in cholesterol levels after the age of 45 and the gender differences observed in the data.
- Describe the exogenous pathway of lipid transport, detailing the role of chylomicrons and the process of dietary cholesterol absorption and transport to the liver and peripheral tissues.
- Understand the endogenous pathway of cholesterol production and transport, explaining how VLDL and LDL function in delivering cholesterol from the liver to peripheral tissues and the impact of HMG-CoA reductase in cholesterol biosynthesis.
- Understand the role of cholesterol in various metabolic processes, including the formation of cell membranes, sex hormones, steroids, bile, and vitamin D.
- Identify the major cardiovascular and endocrine diseases associated with elevated cholesterol levels, such as STEMI, stroke, and hypertension.
- Comprehend the function of low-density lipoproteins (LDL) in transporting cholesterol and triglycerides to tissues and its association with an increased risk of heart disease.
- Comprehend the role of high-density lipoproteins (HDL) in transporting cholesterol from cell membranes back to the liver and its association with a lower risk of heart disease.
Prevalence of High Cholesterol
 |
 |
 |
In western countries, up to two-thirds of the population has a total cholesterol > 5.0 mmol/L. The prevalence of raised cholesterol increases with age up to the 45-54 year bracket with an estimated 81% prevalence in men and 55-64 years for women.
In 2017-18 in Australia, 6.1% of all Australians (1.5 million people) had high cholesterol, which was a decline from 7.1% in 2014-15. The prevalence has fallen to a similar rate to that observed a decade ago in 2007-08 of 5.7%.
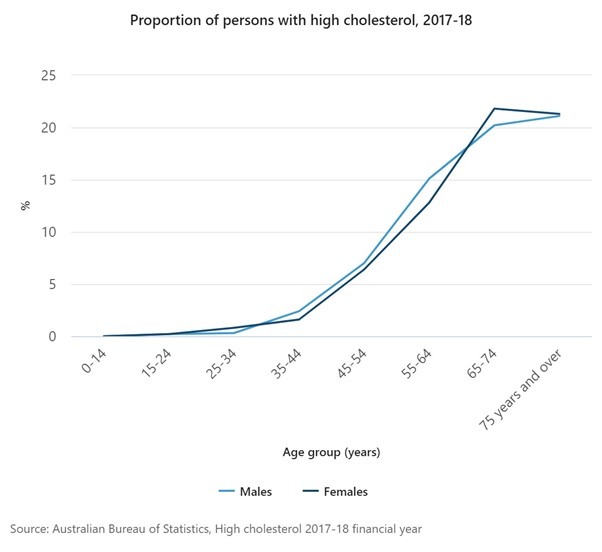
The same proportion of males and females had high cholesterol (6.1%). As with many health conditions, the prevalence of high cholesterol increases with age with a sharp increase from age 45 years. The proportion of people with high cholesterol doubled from age 45-54 years (6.8%) to 55-64 years (14.1%) and increased to one in five people aged 65 years and over (21.2%).
The following two graphs show the sharp rise in people with high cholesterol in 2017-18 – note in the figure below the sharp increase after the age of 44 years for both sexes.
In 2017–18 in Australia, adults aged 18 years and over who were obese were more than twice as likely as adults who were in the normal weight range to have high cholesterol (11.2% compared to 4.5%).
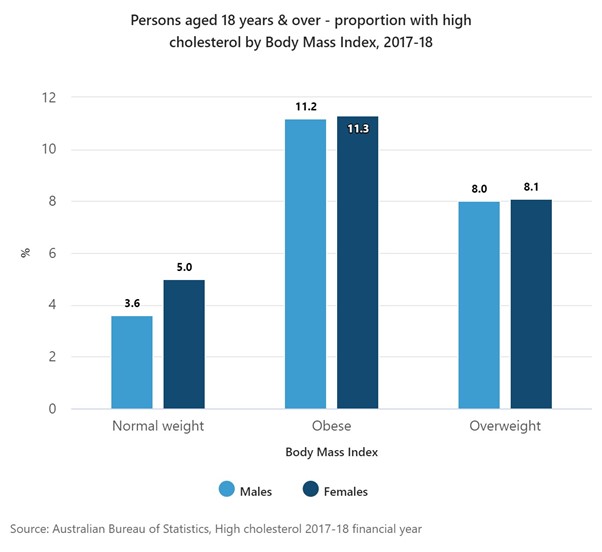
The figure above shows the dramatic association between obesity and elevated cholesterol levels. Obesity is a significant risk factor for cholesterol but also CVD.
📺 Watch video: Hyperlipidemia and epidemiology. (12:53 min)
Lipid Transport and Metabolism
|
|
|
There are two potential sources of cholesterol. The exogenous pathway utilizes dietary cholesterol consumed and absorbed via the small intestine. The endogenous pathway produces cholesterol via hepatic means.
Exogenous pathway (Transport of lipids from GI tract to liver)
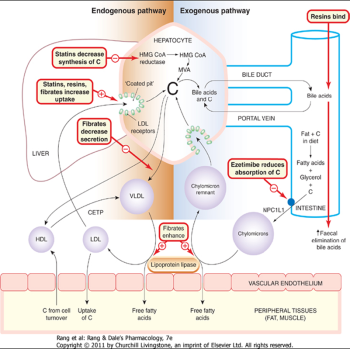
Chylomicrons (‘kylo-microns’) are large particles which transport dietary cholesterol and fatty acids absorbed from the small intestine in the lymph and then blood to capillaries in the muscles and adipose tissue. They consist mainly of tryglycerides (85-95%) and are produced in the small intestine during absorption of a fatty meal. They are cleared from the bloodstream by lipoprotein lipase after 12-14 hours. Lipoprotein lipase then hydrolyses triglycerides and the tissues take up the resulting free fatty acids and glycerol.
The chylomicron remnants (still containing the cholesteryl esters) pass to the liver where they bind to receptors on hepatocytes and undergo endocytosis. Cholesterol liberated in the hepatocytes is stored, oxidised to bile acids, secreted unaltered in bile, or enters the endogenous pathway. The right-hand side of the figure below shows the exogenous pathway. Note the movement of cholesterol to the liver and free fatty acids and glycerol to the peripheral tissues.
Endogenous pathway
Cholesterol and newly synthesised triglycerides are transported from the liver as VLDL (Very Low Density Lipoproteins) to muscle and adipose tissue. The triglycerides are cleaved off by lipoprotein lipase leaving Low Density Lipoproteins (LDL) – the role of LDLs is to transport cholesterol from the liver (initially in the form of VLDL and eventually cleaved to LDL) to peripheral tissues.
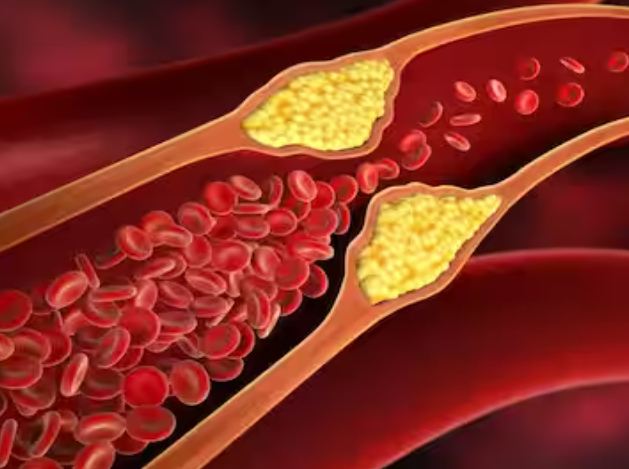
VLDLs contain a large amount of TG (50-65%) and Cholesterol (20-30%). Formed in the liver from endogenously synthesised triglycerides. The triglyceride is hydrolysed to fatty acids and glycerol by lipoprotein lipase. The fatty acids and triglycerides enter the tissues. During this process, the lipoprotein particles become smaller and more dense and retain their cholesteryl esters to form LDL particles. LDL provides the source of cholesterol for incorporation into cell membranes and to synthesise steroids but the transport of excess cholesterol is also key in the development of atherosclerosis.
Endogenous pathway transport of liver-synthesised cholesterol to the peripheral tissues
The liver also produces cholesterol, and this supply of cholesterol can be upregulated or down regulated in response to changes in plasma cholesterol availability. The liver produces cholesterol from Acetyl-CoA. Acetyl-CoA is metabolized to HMG-CoA and then to Mevalonate by the reducing enzyme HMG-CoA reductase.
This is the rate limiting step in the production of cholesterol and is an important target for the statin drug class which reduces endogenous production of cholesterol. The endogenously produced cholesterol is used with the exogenously sourced cholesterol and is used to form bile acid/salts, in the production of Vitamin D and transported to the peripheral tissues by VLDL and LDL.
The figure below shows the important steps in the endogenous production of cholesterol and the role of HMG CoA reductase in the rate limiting step of the formation of Mevalonate from HMG CoA.
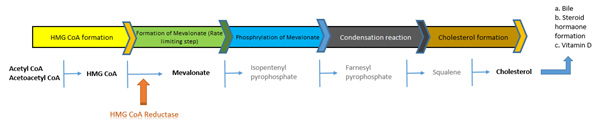
Cholesterol biosynthesis and the potential target of HMG CoA reductase enzyme
📺 Watch video: Lipid transport and metabolism. (8:09 min)
Understanding Lipid Profiles
|
|
|
Cholesterol is used in many metabolic processes. It is used to form cell membranes, sex hormones, steroids, bile and vitamin D (amongst other things). While cholesterol is an important part of normal biological processes, elevated cholesterol represents a major risk factor for a range of cardiovascular and endocrine diseases including but not limited to:
- STEMI (S-T segment elevation myocardial infarction) and Non-STEMI
- Stroke
- Peripheral vascular disease
- Hypertension
- Diabetes.
The relationship between cardiovascular disease and cholesterol is well established. The greater the level of cholesterol, the greater the risk. CVD is one of the most common causes of death in the Western world and over 50% of CVD in Western countries is related to elevated cholesterol levels. To prevent individual and population risks, many drugs have been developed to reduce sustained elevated cholesterol levels to reduce CVD risk.
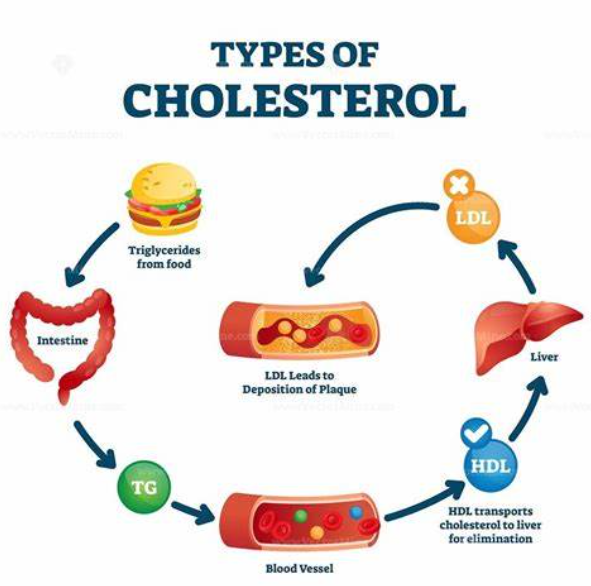
Types of cholesterol.
Cholesterol and triglycerides are water insoluble and need to be transported in plasma within lipoproteins. These lipoproteins transport cholesterol from the liver to the peripheral tissues via VLDL and LDL or transport excess cholesterol from the peripheral tissues back to the liver via the transporter HDL.
Understanding the roles and impacts of LDL, HDL, and triglycerides is critical for managing and preventing cardiovascular diseases. By regulating these lipids through diet, lifestyle changes, and medications, healthcare professionals can significantly improve patient outcomes and overall cardiovascular health.
📺 Watch video: Understanding Lipid Profiles. (6:45 min)
COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING
This material has been reproduced and communicated to you by or on behalf of James Cook University in accordance with section 113P of the Copyright Act 1969 (Act).
The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice.