Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
1.1 Revision of the Anatomy and Physiology of the Cardiovascular System
Revision of the Anatomy and Physiology of the Cardiovascular System
Learning Outcomes
Be able to:
Describe the components and function of blood
Describe the structure and function of the heart
Describe the flow of blood through the heart including the major blood vessels and lungs
Explain how the heart tissue is supplied with nutrients and oxygen
Describe the function of autorhythmic fibres and the electrical conduction system of the heart
Describe the cardiac action potential
Describe how changes in heart rate and stroke volume affect cardiac output
Describe how the central nervous system controls heart rate
Describe the major structural differences between arteries, capillaries and veins.
For this subject, we need to review the three main components of the cardiovascular system. These include the:
1. Blood
2. Heart, and,
3. Vasculature.
1. The Blood
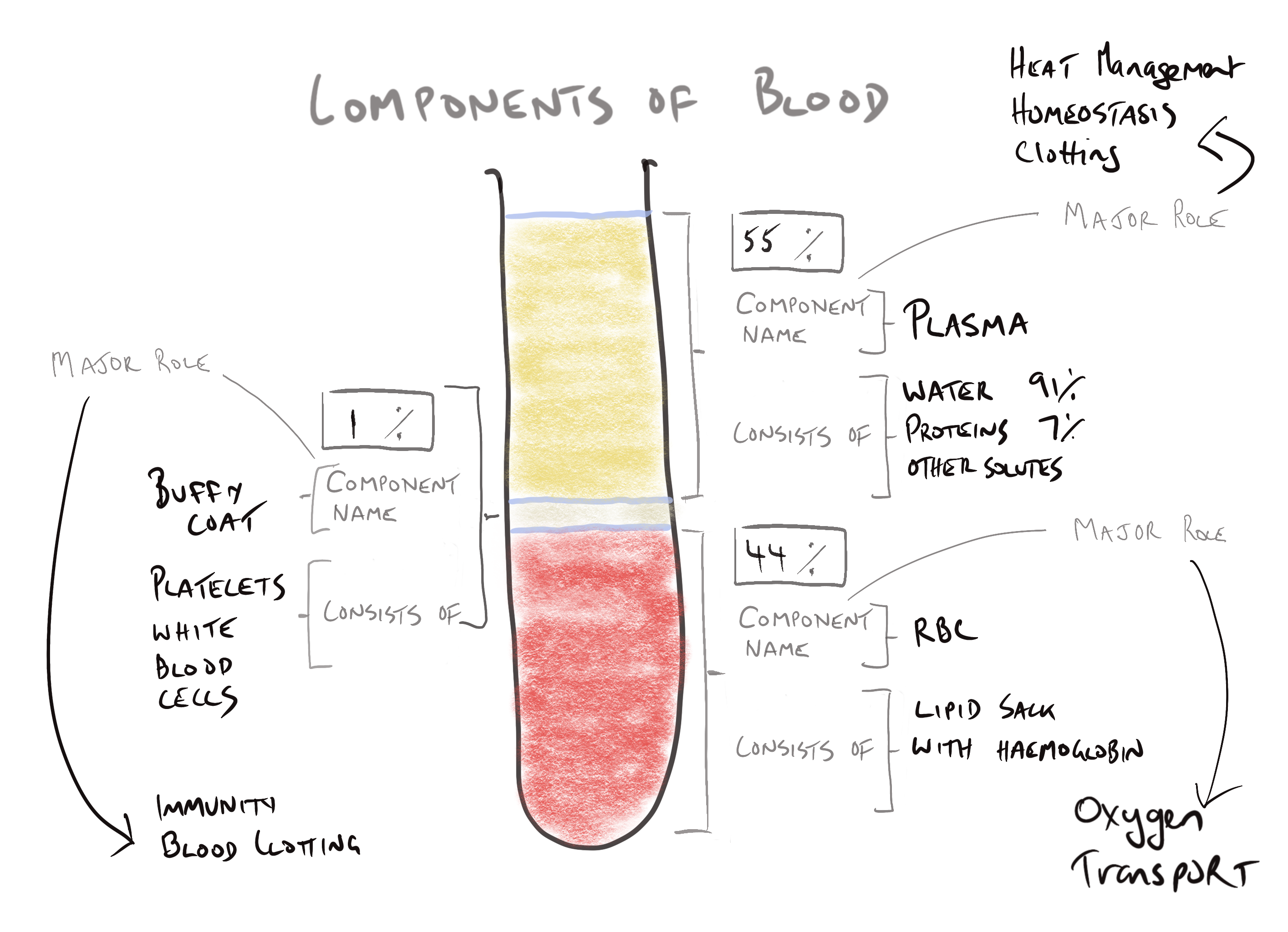
Cells and multicellular organs are immobile and cannot obtain and exchange oxygen and metabolic waste products without the aid of blood and interstitial fluid which bathes the cells and assists with oxygen, nutrient and waste exchange. Interstitial fluid represents the majority of extracellular fluid (around 80%), is the exchange medium between the cell and blood contained in the blood vessels and is replenished by the blood. Blood in its simplest composition consists of 2 main parts. These are the plasma and the formed elements.
Plasma consists of about 55% of the volume of blood. The plasma contains mostly water (more than 90%) and the proteins found in blood (albumin, globulins [different globulins have an oncotic, immune and clotting function], fibrinogen and other proteins), solutes such as electrolytes, gases and waste products.
Image adapted from Interactive figure 19.1 – Components of blood in a normal adult in Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 available athttps://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/52!/4/2/2/26@0:0
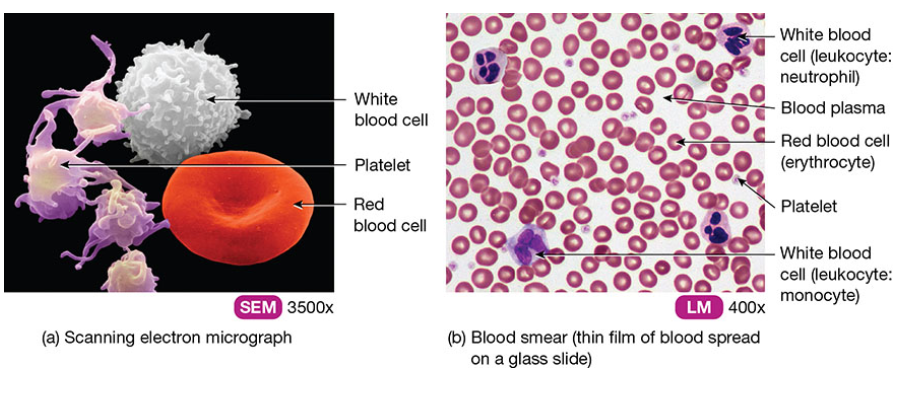
The other 45% of blood contains the formed elements. Red blood cells (RBCs) make up the vast majority of the formed elements (44% of the total blood volume). RBCs are also known as erythrocytes and are responsible for the transport of oxygen in the blood. Red blood cells have a very flexible plasma membrane that also displays surface glycolipids that act like antigens and account for the different blood groups. RBCs do not have a nucleus or other organelles typically found in cells, instead, it has a haemoglobulin molecule which contains four iron containing haem groups. A lay description of a RBC might be this… a RBC is simply a bag of haemoglobin useful for transporting oxygen through the blood.
The remaining component of the formed component of blood is white cells (neutrophils, lymphocytes, monocytes, eosinophils and basophils) important in providing immunity and platelets (aka thrombocytes), responsible for the initiation of clotting of blood during bleeding.
This layer is often white when centrifuged down and is termed the ‘buffy layer’. It represents about 1% of the total blood volume. The figure below shows a) a scanning electron micrograph of RBCs, platelets and white blood cells and b) a 400x magnification of blood through a microscope again showing the red blood cells, platelets and stained white blood cells.
The last major function of blood is to maintain homeostasis of body fluids, regulate pH through the use of buffers, influence the water content of body cells by maintaining relevant oncotic pressure and assist in cooling the body (water is a good heat conductor and allows for heat to be transported to the surface of the body for loss to the environment).
So, the three main functions of blood is:
Transportation of oxygen;
Provide immune function via white blood cells and clotting via platelets; and
Regulate homeostasis of body fluids (including the regulation of heart.
And, in summary,
Blood and lymphatic fluid are essential to provide oxygen and nutrients to cells and organs and remove metabolic waste products.
Blood has 2 major components – the first is the plasma which contains mostly water with some electrolytes, dissolved gasses and proteins such as albumin. The second is the formed component which are made up of (mostly) red blood cells, white cells and platelets.
The 3 major functions of blood are oxygen transportation and cellular waste removal, transportation of immune cells to target areas and regulation of homeostasis (including heat regulation).
Check your understanding #1
Check your understanding #2
The following figure shows a sample of 20ml of blood after it was spun down in a centrifuge revealing the 3 major component parts. Complete the following diagram providing detail about the different components and role of each of the major components of blood.
Revise Section 19.1 Functions and Properties of blood in Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G.,Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 available at https://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/52!/4/2/2/8@0:0.
2. The Heart
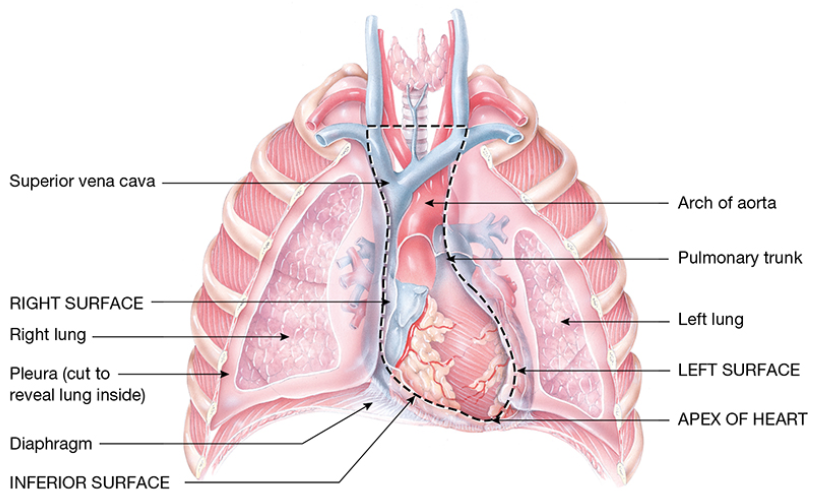
The heart is located in the mediastinum between the left and right lungs near the midline of the thoracic cavity. Two-thirds of the bulk of the heart lies on the left side of the midline.
Anterior view of the heart and thoracic cavity. Figure 20.1b taken from Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019.
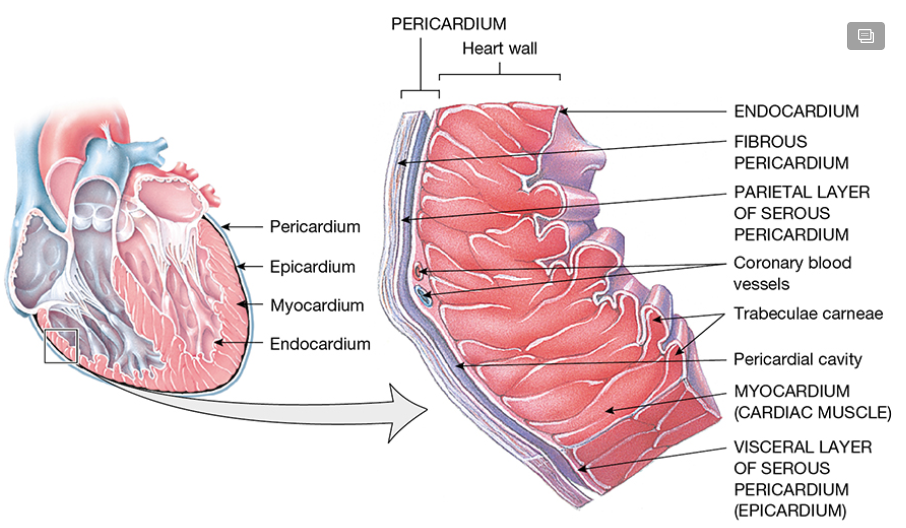
The heart is surrounded by a locating and protective structure called the pericardium. The pericardium has two parts, the fibrous pericardium, an outer fibrous sac that protects the heart and anchors it at the location of the diaphragm and the epicardium (aka serous epicardium) that reduces friction with surrounding structures when the heart beats within the chest cavity.
The tissue of the outer pericardium is dense, non-elastic and irregular. Its main purpose is to provide a protective sheath and stop the heart from over-stretching. Between the outer layer of the pericardium and heart itself is a double layer of serous pericardium – also known as the epicardium. The epicardium secretes serous fluid that provides lubrication and reduces friction during movement of the heart. The space between the two layers of serous pericardium (which is also between the outer surface of the heart and the outer pericardium is called the pericardial cavity. It is the pericardial cavity that contains the pericardial fluid.
Portion of the pericardium and right ventricular heart wall showing divisions of pericardium and layers of heart wall. Figure 20.2a from Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019.
The myocardial tissue (heart tissue) consists of 3 layers. From outside to inside, the layers are the epicardium, myocardium and endocardium. The epicardium (serous pericardium) we have already learned about. The endocardium is the innermost layer of tissue of the heart. The innermost endocardium layer is essentially a thin epithelial layer of the innermost surface of the chambers of the heart and valves that provides a smooth surface for blood to minimise surface friction. The middle layer (the myocardium or heart muscle) is responsible for the pumping action of the heart and makes up the majority of the heart tissue.
The heart has four main chambers: 2 atria and 2 ventricles. Watch the short animation below on the movement of blood through the heart then return here to read on…
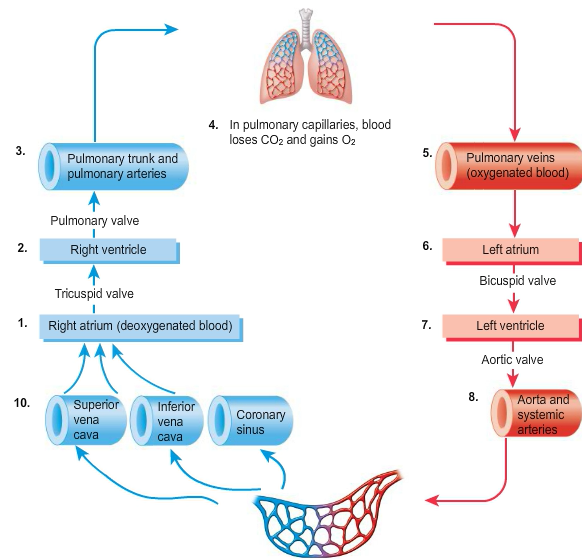
Welcome back!… The right atrium [1] receives deoxygenated blood from the circulation via the superior and inferior vena cava. Contraction of the right atrium sends blood to the larger right ventricle [2] via the tricuspid valve (so called as it has 3 flaps making up the valve. Contraction of the right ventricle sends blood to the lungs for oxygenation past the pulmonary valve via the left and right pulmonary arteries [3]. After gas exchange has occurred in the lungs at the site of lung capillaries and alveolar [4], the now oxygenated blood returns to the left atrium [6] via the left and right pulmonary veins [5] where it is sent to the left ventricle [7] via the mitral valve (a bi-flap valve). Contraction of the left ventricle sends oxygenated blood through the aortic valve to the ascending aorta [8] for circulation to the capillary beds in the various tissues around the body [9].
Path of blood flow through systemic and pulmonary circulations. Interactive Figure 20.7 from Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019.
📚 Read/Explore
Revise section 20.1 – Location of the heart and Pericardium in your anatomy and physiology text: Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 available at https://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/54!/4/2/2/8/6/4@0:0.
Revise section 20.1 – Layers of the heart wall in your anatomy and physiology text: Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 available at https://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/54!/4/2/2/30/4/8/2/2@0:0.
Revise section 20.1 – Chambers of the heart in your anatomy and physiology text: Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 available at https://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/54!/4/2/2/40/4@0:100.
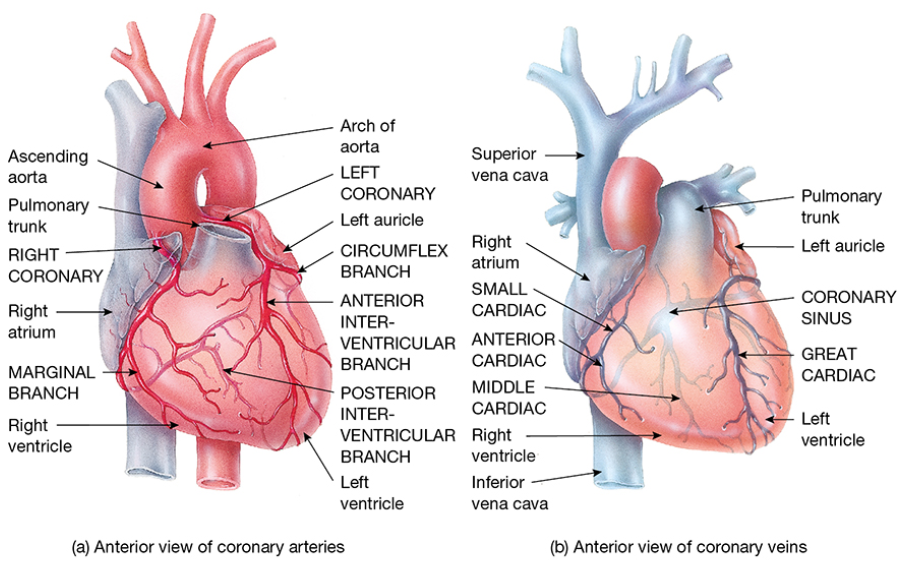
Blood supply to the myocardial tissue is provided by the coronary arteries. There are two main coronary arteries, the right coronary artery which supplies the right atrium and right ventricle muscle, the septum and the sinu-atrial node. The left main coronary artery supplies the left anterior atrium and ventricle via the left anterior descending artery and the circumflex artery supplies the posterior left atrium and ventricle. The oxygenated blood supply for the left and right coronary arteries come from the base of the aorta. There is a corresponding system of coronary veins which take the deoxygenated blood and waste products from the myocardial tissue and deposits the blood back into the right atrium via the coronary sinus. The interesting thing to know here is this is how heart attacks happen. Interesting fact: A heart attack (aka myocardial infarction) occurs when one or more of the coronary arteries is blocked, causing a reduced blood supply to the myocardium (heart muscle) – so you don’t need to know which coronary artery supplies the different sections of the heart, but it is useful to know the function of coronary arteries.
Image from Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019.
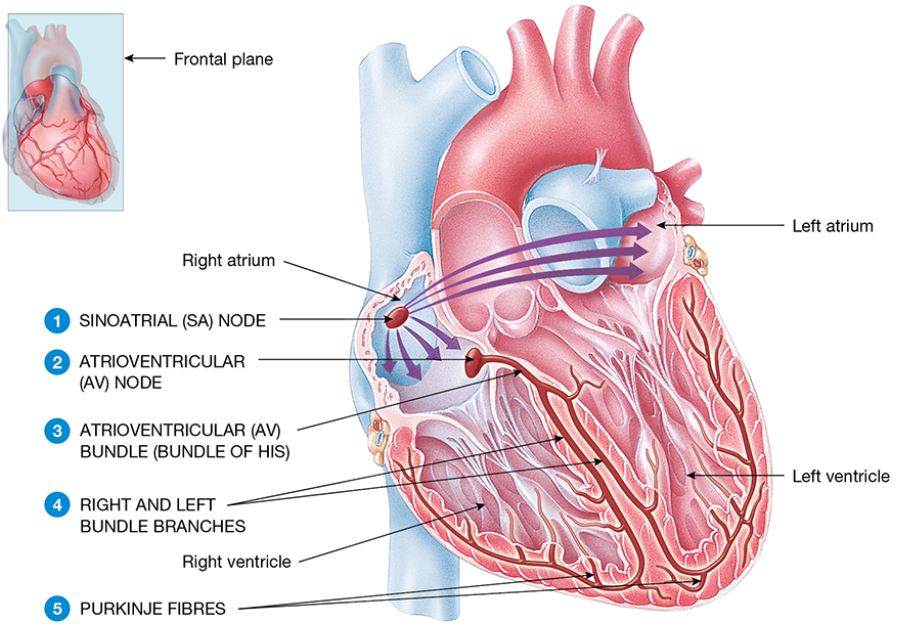
The continuous and rhythmic contraction of the heart tissue is under the control of autorhythmic fibres of the electrical conduction system in the heart. Cardiac tissue contraction should begin with the sinoatrial (SA) node (located in the superior vena cava) depolarising reaching threshold potential [1]. The SA node acts as a pacemaker and has no stable resting potential, so it repeatedly and predictably depolarizes triggering an action potential in the right and left atrial tissue.
The atrial tissue passes the electrical signal to the atrioventricular (AV) node [2]. The AV node slows the conduction rate to allow the two atria to contract fully and push the blood into the ventricles. The delayed signal is passed onto the bundle of His [3] and the right and left bundle branches [4] and eventually the purkinje fibres [5]. This causes the depolarization of the skeletal muscle and contraction of the right and left ventricles. This forces the blood from the ventricles to the lungs via the pulmonary arteries or the systemic circulation via the aorta.
Image from Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019.
📚 Read/Explore:
Revise coronary circulation in your anatomy and physiology text: Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 available at https://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/54!/4/2/2/112@0:0.
Revise Histology of cardiac muscle tissue and Autorhythmic fibres: the conduction system in your anatomy and physiology text: Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 available at https://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/54!/4/2/2/138/6/2@0:24.5
The initiation of the action potential from the SA node onto other nodal tissue is eventually passed onto the contractile muscle tissue of the heart. The action potential from the SA node is passed onto the first myocardial fibre via the electrical conduction system of the heart.
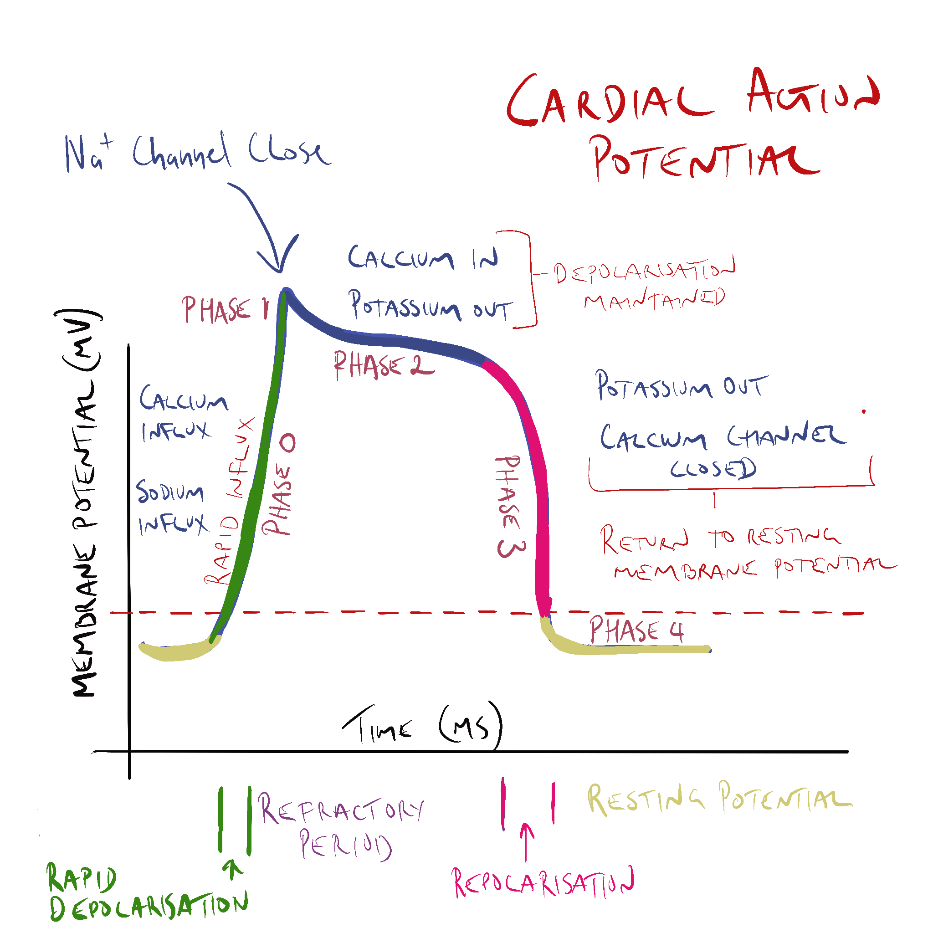
Phase 4 – Yep, it starts with phase 4!?! The action potential starts with phase 4 of the cardiac cycle where the transmembrane potential is less than -90 mV and is maintained there by a slow but constant leak of potassium ions (K+) from the cardiac myocyte. Sodium and calcium channels are closed. The cardiac myocyte has a stable resting membrane potential of less than -90 mV.
Phase 0 – When the transmembrane potential rises above -90 mV, fast sodium channels begin to open slowly one by one allowing positively charged sodium ions to trickle in and reduce the transmembrane potential to -70 mV – the threshold potential of cardiac myocytes. Once this threshold has been reached, more fast sodium channels open allowing a rush of sodium into the myocyte reducing the transmembrane potential. At -40 mV, the L-type calcium channels open allowing a small but steady influx of calcium (Ca2+) into the cell. The sodium influx causes an overshoot of the transmembrane potential past 0 mV. The fast sodium channels close.
Phase 1 – the slightly positive transmembrane potential is corrected by the opening of potassium channels briefly allowing the outward movement of K+ ions out of the cardiac myocyte.
Phase 2 – L-type calcium channels remain open allowing a constant inward movement of calcium ions. This is significant for the excitation-contraction coupling process which causes the physiological contraction of myocytes. At the same time, potassium is continuing to leak out of the cell. The balance between the inward movement of Ca2+ and the outward movement of K+ maintains a plateau just below 0 mV.
Phase 3 – in phase 3, the calcium channels are closed, the persistent outflow of potassium (K+) sends the transmembrane potential back towards its resting membrane potential of -90 mV awaiting the next cycle of depolarization. Normal pre-depolarisation ions concentrations are corrected and ready for the next action potential.
The myocytes are electrically coupled through gap junctions so one myocyte passes on the action potential to the next. This couples all of the individual myocytes to produce a contraction on an organ scale.
Cardiac action potential and the movement of most important ions at the different phases of the cardiac action potential.
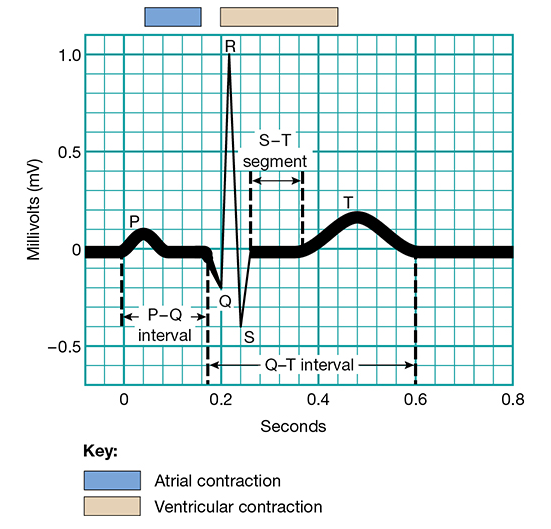
The depolarization of the myocardial tissue (as a linked bunch of myocytes) can be measured using an electrocardiogram (ECG). The ECG is useful to identify abnormalities in conduction within the heart and a normal ECG displays a P-QRS-T pattern. The P-wave reflects depolarization (contraction) of the left and right atria. The QRS indicates ventricular contraction and the T-wave ventricular repolarization.
Image from Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019.
📚 Read/Explore
Revise section 20.3 – Action potential and contraction of contractile fibres in your anatomy and physiology text: Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 availabnle https://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/54!/4/2/2/176/4/4/2@0:69.9.
Revise section 20.3 – Electrocardiogram and Correlation of ECG waves with atrial and ventricular systole in your anatomy and physiology text: Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 available athttps://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/54!/4/2/2/198@0:32.4.
Cardiac output (CO) is very important. Cardiac output is a measure of the volume of blood the heart is able to circulate in one minute. It is governed by two factors – stroke volume (SV) – the volume of blood ejected by either ventricle (depending on which one is being measured) in a single contraction. On average, this is about 70ml for a normal adult male. The second factor affecting cardiac output is heart rate – assuming a heart rate of 75 beats per minute (bpm) cardiac output (CO) can be calculated as follows:
📚 Read/Explore
Revision activity: Go to the following website and calculate your blood volume – https://www.omnicalculator.com/health/blood-volume. Take your pulse and measure your heart rate Assume a SV of 70ml for both males and females. Calculate your cardiac output. Calculate the % of total blood volume that is circulated each minute.
Revision activity: What happens to cardiac output when heart rate increases during exercise?
Revision activity: During heart failure, ventricular hypertrophy occurs. Because the heart is somewhat restricted in physical size, the muscle grows both outward (to an extent) and inward, reducing the volume of the ventricular chambers. What do you expect would happen to cardiac output during ventricular hypertrophy as a result of heart failure?
Revise section 20.5 – Cardiac output in your anatomy and physiology text: Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 available athttps://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/54!/4/2/2/304@0:0.
The tissue within the heart that has the highest automaticity rate is the SA node. Most tissue, including the AV node and even the myocardial tissue has some automaticity potential, but in normal function, it is much lower than the SA node. This means it is the SA node that is the dominant pace maker and sets heart rate. If the SA node is not influenced by the sympathetic or parasympathetic systems, the average rate of spontaneous depolarization around every 0.6 seconds or approximately 100 times a minute.
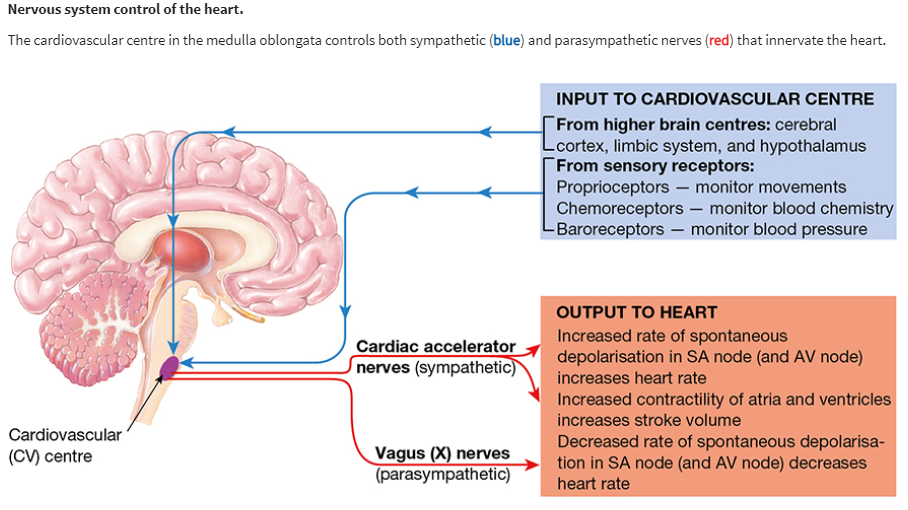
This can be regulated by the sympathetic and parasympathetic system under the control of the Cardiovascular Centre (CV) in the medulla oblongata. The cardiac centre takes input from the higher brain centres and sensory receptors around the body (proprioceptors, chemoreceptors and baroreceptors) and regulates heart rate and contractility by changing the rate of sino-atrial node firing. It can increase heart rate it via the cardiac accelerator nerves of the sympathetic nervous system releasing adrenaline and (mostly) noradrenaline) or decreasing the rate of spontaneous depolarization of the SA and AV nodes via the release of acetylcholine from the Vagus nerve of the parasympathetic nervous system.
The release of noradrenaline from the cardiac accelerator nerves interact with beta-1 receptors on the SA and AV node and myocardial tissue to increase rate of SA and AV node firing and to increase the influx of calcium into the myocardial cell to increase contractile force.
Conversely, the release of acetylcholine from the Vagus (X) nerve at the SA and AV node (and atrial myocardium) decreases the rate of firing of the autorhythmic fibres in that tissue.
Note: the description at the top of this diagram is wrong. Ignore it.
Image from Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019.
Check your understanding #3
3. Blood Vessels
There are five main types of blood vessels (in order of flow): arteries –> arterioles –> capillaries –> venules –> and veins. Arteries branch into smaller arteries and even smaller arterioles before reaching the capillary bed where waste, oxygen and nutrients are exchanged with cells. The capillaries unite in venules, smaller veins and eventually large veins. Arteries are defined simply as vessels that carry blood from the heart and veins are vessels that carry blood to the heart (note: it is not defined by oxygenated and unoxygenated blood though in most cases arteries carry oxygenated blood and veins deoxygenated blood).
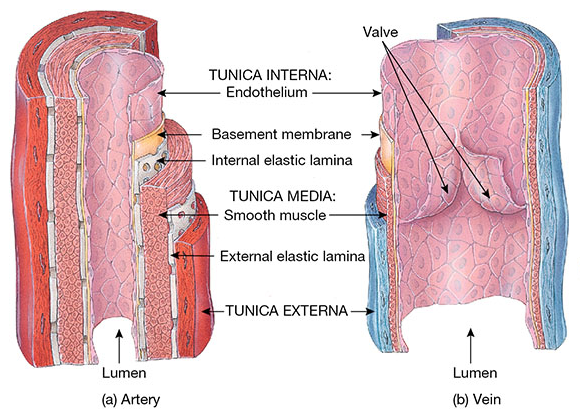
Both arteries and veins share structural similarities. An external sheath called the tunica externa, a layer of smooth muscle (the tunica media) and an internal layer of endothelium called the tunica interna.
Image from Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019.
As you can see from the diagram above, arteries have a thicker outer and middle layer with large amounts of elastic fibres allowing for stretch of the vessel. This allows for the continued forward movement of blood during diastole and accommodation of the surge of blood during systole. As a general rule, the smaller the arterial vessel the less elasticity.
The capillaries are much thinner walled vessels that allow for exchange of nutrients and waste. Capillary structure differs from that of arteries and veins. They have no tunica externa or media and consist solely of a very narrow diameter lumen consisting only of endothelial cells.
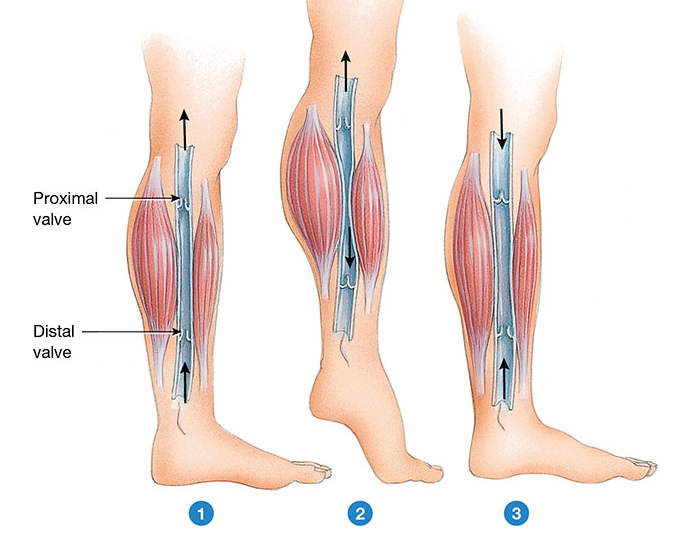
Veins have much thinner walls and do not change as much in structure according to size unlike arteries. The external and middle layers of the vein is much thinner than arteries and while they are distensible to a degree, they are not designed for high pressure environments. Veins rely on the pressure generated by the heart to continue circulation through the body. To aid this, the flow of blood from the lower peripheries is also facilitated by the contraction of skeletal muscles in the legs. To stop back flow in the peripheries, many veins also contain valves to prevent backflow of blood in the vessel.
Image from Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019.
📚 Read/Explore
Revision activity: What is an example in the body where a vein caries oxygenated blood and a artery carries deoxygenated blood?
Revise section 20.5 – Arteries in your anatomy and physiology text: Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 available at https://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/56!/4/2/2/38/12@0:100.
Revise section 20.5 on capillaries in your anatomy and physiology text: Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 available at https://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/56!/4/2/2/76@0:0.
COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING
This material has been reproduced and communicated to you by or on behalf of James Cook University in accordance with section 113P of the Copyright Act 1969 (Act).
The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice.
Image adapted from Interactive figure 19.1 – Components of blood in a normal adult in Tortora, GJ., Derrickson, B., Burkett, B., Peoples, G., Dye, D., Cooke, J., et al. Principles of anatomy and physiology. Second Asia-Pacific ed. Queensland, Australia: John Wiley & Sons; 2019 available at https://bookshelf.vitalsource.com/#/books/9780730354987/cfi/6/52!/4/2/2/26@0:0
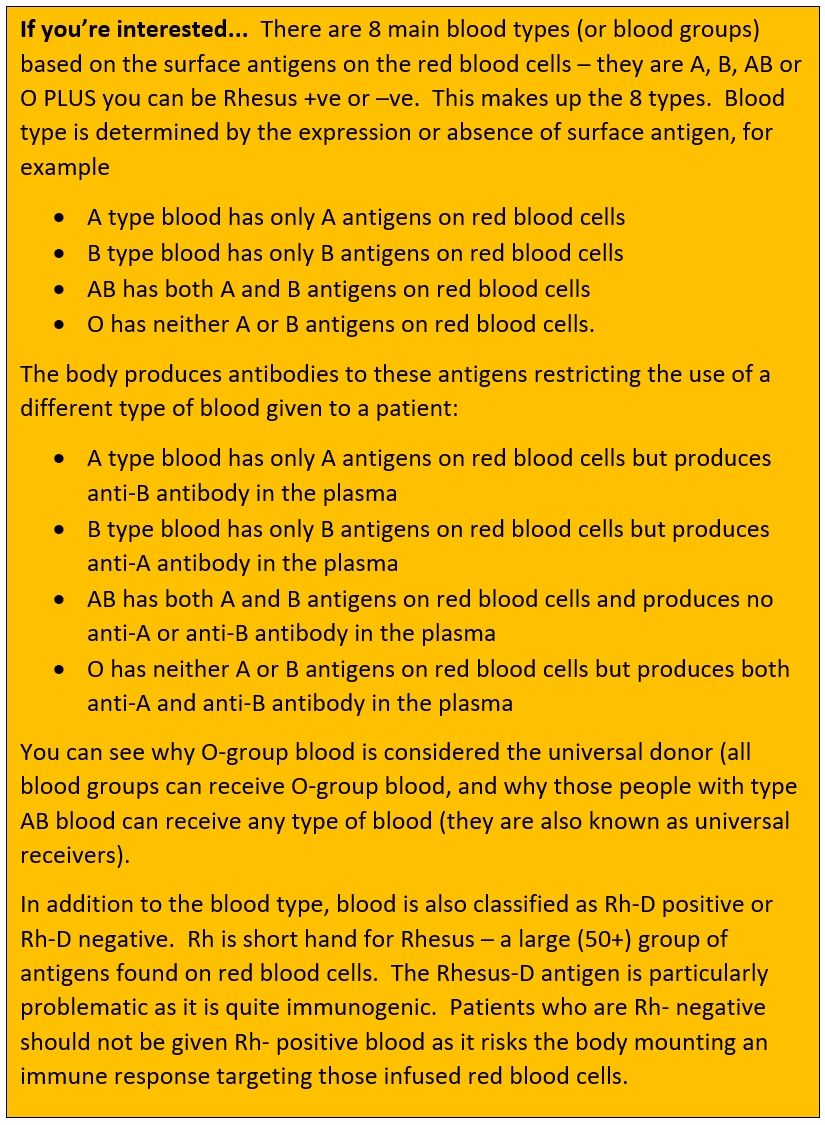 If you’re interested – Blood types explained
If you’re interested – Blood types explained