Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
2.2.2 Overall Management for Elevated Cholesterol
Learning Outcomes
Be able to:
Determine whether to treat elevated cholesterol levels in patients based on their individual cardiovascular risk, and identify the appropriate cholesterol-lowering targets for high, intermediate, and low-risk patients.
Assess cardiovascular risk using the AusCVDRisk tool, which includes factors such as age, gender, smoking status, cholesterol ratio, systolic blood pressure, diabetes, medication use, history of atrial fibrillation, and socioeconomic status, and apply intensive lifestyle advice and pharmacotherapy accordingly.
Treatment for Elevated Cholesterol Based on Patients AusCVD Risk
Case Study: Alf Landerman
Alf is a 55-year-old Indigenous man well known to you who presents for a well man check-up. Alf works for the Cairns Airport as an air traffic controller. He lives with his wife Cynthia and one child.
Patient: Alf Landerman, 55-year-old Indigenous male
Medical History:
Quit smoking 5 years ago
Systolic blood pressure: 145 mmHg
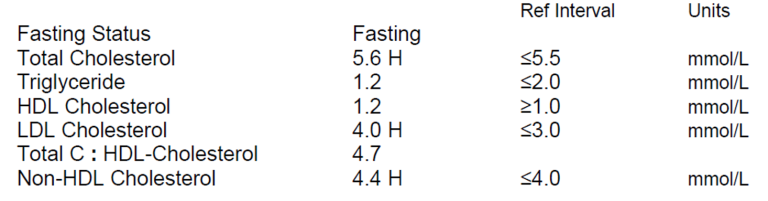
Total cholesterol: 5.5 mmol/L
HDL cholesterol: 1.2 mmol/L
Currently takes ramipril 10mg OD in the morning for elevated blood pressure
No history of atrial fibrillation (AF), diabetes, kidney disease, or familial hypercholesterolemia
Location: Cairns, QLD 4870
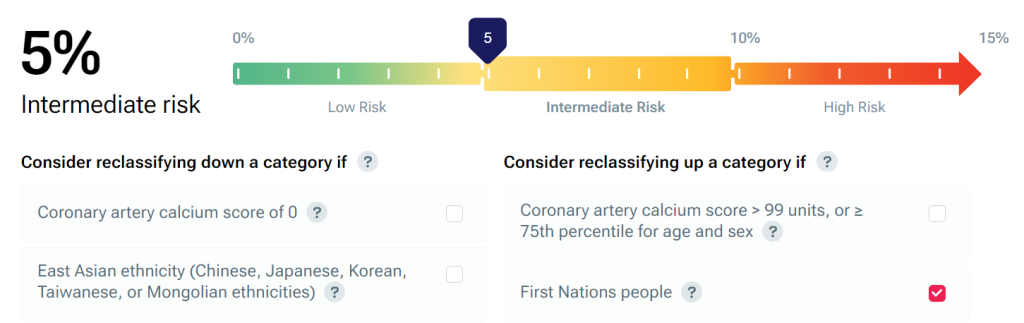
Alf has a intermediate risk of CVD in the next 5 years, but as he is an Indigenous man, his risk has been elevated by one category to high risk.
So, the question is – do we treat Alf’s elevated cholesterol levels? If so, what are our agreed cholesterol lowering targets and how do we reduce his cholesterol and monitor progress?
Let’s leave the how and monitoring for a later section. Let’s focus on the ‘do we treat’ and ‘what are the targets’ part of the problem.
The approach to cholesterol lowering is based on the individual’s CV risk
The risk of the individual patient developing cardiovascular disease in the next 5 years directs the therapeutic approach to the management of diabetes. Adults without established cardiovascular disease who are 45 years or older (or 30 years or older if Aboriginal and Torres Strait Islander) should have their CV risk calculated.
Patients with established cardiovascular disease do not need their risk calculated as they are at high risk by virtue of having established CV disease. These people will benefit from an absolute risk reduction strategy as they will be in the high risk (or very high) category. Remember that we are providing secondary prevention in these patients and the associated treatment targets are often lower (more aggressive treatment) compared to primary prevention.
Back to primary prevention – CV risk in Australia is calculated using the AusCVDRisk tool. This tool considers:
Age
Gender
Smoking status
Cholesterol ratio
Systolic blood pressure
Diabetes
Use of medication
History of atrial fibrillation
Socioeconomic status.
Presented as a 5-year risk as a percentage. It calculates the risk and stratifies the risk into 3 categories: high risk, intermediate risk and low risk.
Patients with a high risk of CV disease in the next 5 years
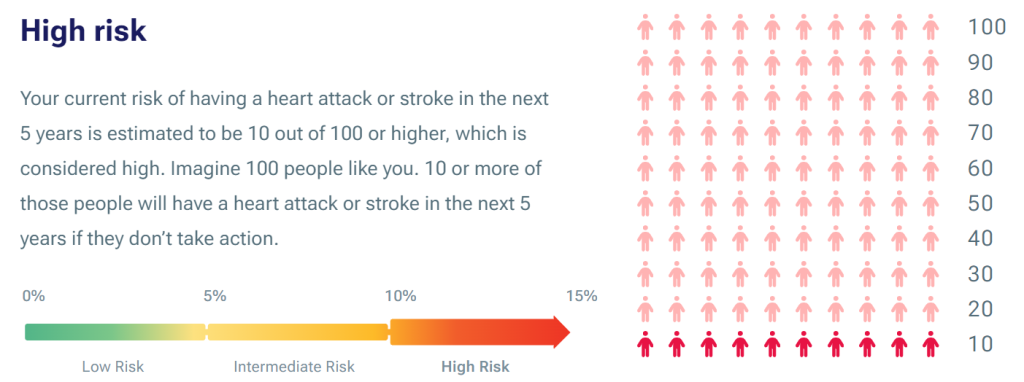
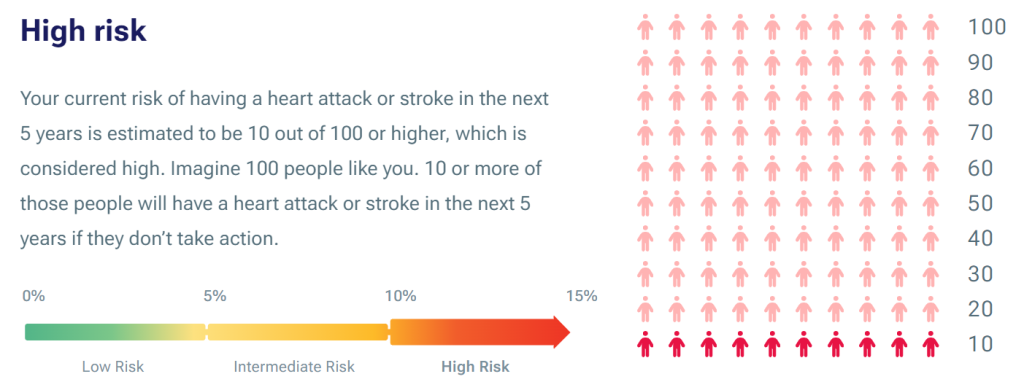
Based on Alf’s high risk of cardiovascular risk in the next 5 years (let’s assume 10%), he is at high risk of developing cardiovascular disease in the next 5 years. Patients in the high risk group should be provided intensive lifestyle advice aimed at lowering cholesterol and blood pressure as well as pharmacotherapy for cholesterol and blood pressure.
Patients with an intermediate risk of CV disease in the next 5 years
Patients with an intermediate risk should be considered for reclassification as either low or high risk. If after consideration they remain at intermediate risk, they should be provided with intensive lifestyle advice and considered for pharmacotherapy considering overall CV risk, patient preferences and benefits and risks.
Patients with a low risk of CV disease in the next 5 years
Patients with elevated cholesterol with a low absolute risk of developing cardiovascular disease in the next 5 years should be provided lifestyle advice to reduce lipid levels naturally and repeat the lipids every 5 years. Lifestyle modifications known to reduce cholesterol include:
Weight reduction – a 2.3kg loss in body weight can double the lipid lowering effect of dietary modification alone, it also reduces the rate of production of VLDL (and thus LDL), decrease triglyceride levels and slightly increase HDL cholesterol. The target BMI should be > 25.
Dietary modification – intensive dietary intervention can decrease total cholesterol and LDL cholesterol by up to 30%. The general aim of dietary modification is to decrease the intake of saturated fat and cholesterol containing foods and increase the proportion of polyunsaturated and monounsaturated fat, consume moderate amounts of lean meats, fish, eggs, tofu, nuts and seeds, dairy such as milk, yoghurt and cheese, moderate amounts of fruit and a larger proportion of vegetables, legumes and beans and larger proportion of grains and cereals. Dietary modification can also enhance the effects of lipid lowering drugs. Visit the following link to review the Australian Guide to Healthy Eating.
Alcohol reduction or elimination – there is a linear relationship between serum triglyceride levels and increased alcohol consumption. The effect of alcohol upon HDL cholesterol is less certain with some patients experiencing an increase in HDL-C and some a reduction in HDL-C.
Smoking cessation – smoking increases plasma cholesterol levels with an association between each cigarette and a subsequent increase in plasma cholesterol levels.
Treatment Targets
Targeting CVD risk assessment to recommended age groups enables people at high risk of CVD to be identified early before they develop overt disease. This approach helps direct pharmacological strategies for intensive CVD risk factor management to people at high risk and diverts unnecessary interventions away from people at lower risk. Cardiovascular disease (CVD) risk assessment and management in people without known CVD involves:
identifying the appropriate people to be assessed;
using the Australian cardiovascular disease risk calculator (Aus CVD Risk Calculator) to estimate their risk;
identifying their risk category (see below);
communicating their risk to them; and managing their risk.
Irrespective of the management approach, for example non-pharmacological (SNAP and weight management) approach, or drug and non-drug approach, we need a target in mind to aim for. The information below provides targets for cholesterol levels based upon level of risk.
Now, understanding this, let’s reconsider Alf. You will remember Alf’s CVD risk over the next 5 years was 10% (we elevated the category due to his Indigeneity).
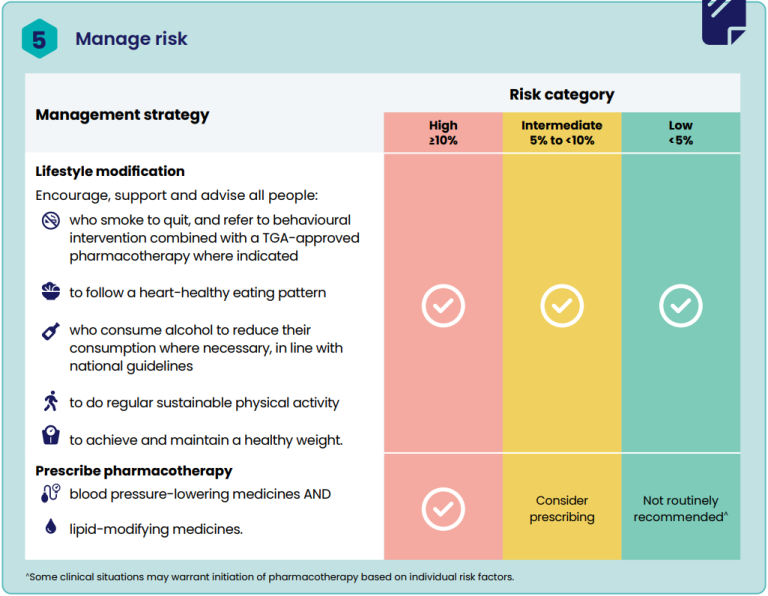
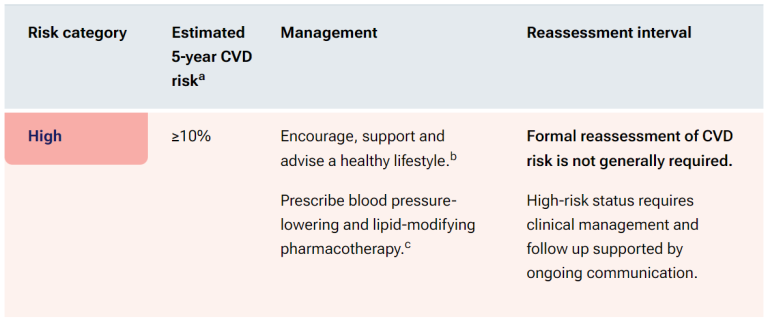
If we consult the AusCVD risk guideline and look at the Overview of CVD risk management according to risk category, we would find the following information:
According to the treatment strategy, we would:
Commence lifestyle changes PLUS
Commence lipid lowering drug therapy.
We would target Alf’s cholesterol level to which of the following? If we consider the information on target cholesterol levels, we would be aiming for the following cholesterol levels:
LDL-C target: At least 50% reduction in LDL-C from baseline and less than 1.8 mmol/L, whichever is lowest
non–HDL-Ctarget: less than 2.6 mmol/L
triglycerides target: less than 1.7 mmol/L
… remember, the relationship between cholesterol levels and CVD risk is continuous, that is the lower the cholesterol level, the lower the risk… so we try to get it to target level, but any progress towards that level is better than no progress at all.
📺 Watch video: Lipid targets. (1:34 min)
Non-Drug Treatment Used to Manage Dyslipideamia
Lifestyle changes have been proven to play a crucial role in managing dyslipidaemia, reducing total cholesterol (TC), low-density lipoprotein (LDL) cholesterol levels, and atherogenesis. Research indicates that a combination of complete smoking cessation, maintaining a body mass index (BMI) below 22, and achieving a simulated mean cholesterol level of 2.3 mmol/L can halve the 12-year risk of coronary heart disease (CHD) in both men and women.
Weight Loss
Weight loss plays a significant role in reducing cholesterol levels. A 2.3 kg loss in body weight can double the lipid-lowering effect of dietary modification alone. Weight loss reduces the rate of production of very low-density lipoprotein (VLDL) cholesterol in the liver, which subsequently lowers the production of LDL cholesterol. It can also reduce triglyceride levels and slightly increase high-density lipoprotein (HDL) cholesterol levels. People with hyperlipidaemia who are overweight or obese should aim to reduce their BMI to 25 or less unless contraindicated.
Smoking Cessation
Smoking cessation is another critical factor in managing cholesterol levels. Increasing levels of plasma cholesterol concentration are associated with an increasing number of cigarettes smoked. For instance, in men aged 18-60 years, the average plasma concentration of cholesterol increases by 0.0085 mmol/L for each cigarette smoked, and in women aged 31-50 years, it increases by 0.0124 mmol/L per cigarette. This association is not observed in men and women over 60 years of age.
Dietary Modification (Nutrition)
Dietary modification is an essential part of managing lipid disorders and can significantly improve dyslipidaemias. Intensive dietary intervention can decrease total cholesterol and LDL cholesterol by up to 30%. The general aim of dietary modification is to decrease the intake of saturated fat and cholesterol while increasing the proportion of polyunsaturated fat in the diet. This approach can enhance the therapeutic effects of lipid-lowering drugs and, in some cases, be as effective as certain statins.
Alcohol Consumption
Alcohol consumption has a linear relationship with serum triglycerides. Excessive alcohol intake worsens dyslipidaemia in patients with raised triglyceride levels. There is also a relationship between HDL cholesterol concentrations and alcohol consumption; increased alcohol consumption raises plasma HDL cholesterol concentrations. However, patients with underlying dyslipidaemia can still have a low HDL cholesterol level even with high alcohol intake.
Physical Activity
Physical activity has been shown to raise HDL cholesterol levels. Greater increases in physical activity result in more significant rises in HDL cholesterol. Aerobic exercises, such as brisk walking, cycling, jogging, and swimming, for 30 minutes 3-5 times per week, have demonstrated a desirable effect on the lipid profile.
In conclusion, incorporating lifestyle changes such as dietary modification, weight loss, smoking cessation, moderated alcohol consumption, and increased physical activity can substantially improve cholesterol levels and reduce the risk of cardiovascular diseases.
📺 Watch video: Non-drug interventions to reduce cholesterol. (14:03 min)
Introduction to Common Drugs Used to Manage Dyslipideamia
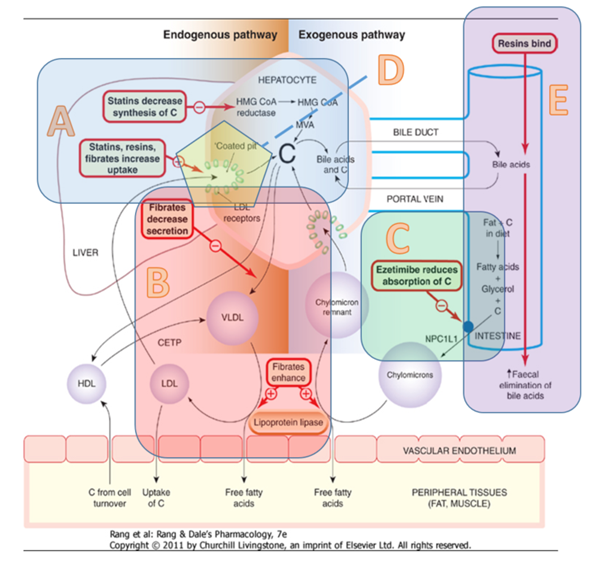
There are 4 main drug classes that can reduce plasma cholesterol levels:
Statins – Statins decrease the body’s internal production of cholesterol. (Refer to A in the figure below).
Fibrates – Fibrates increase lipolysis in the tissues (Refer to B in the figure below).
Ezetimibe – Ezetimibe inhibits brush border enzymes reducing the absorption of cholesterol (Refer to C in the figure below).
PSCK9 inhibitors – PSCK9 inhibitors decrease the breakdown of LDL receptors in the liver increasing scavenging of cholesterol from the blood.
Note that the 4 main drug classes, as they work in different ways, a combination of 2 or more of these medications can lower cholesterol more than one medicine alone.
Site of action of the different classes of drugs used to lower cholesterol (A: statins, B: Fibrates, C: Ezetimibe, D: PCSK9 inhibitors and E: Bile acid binding resins
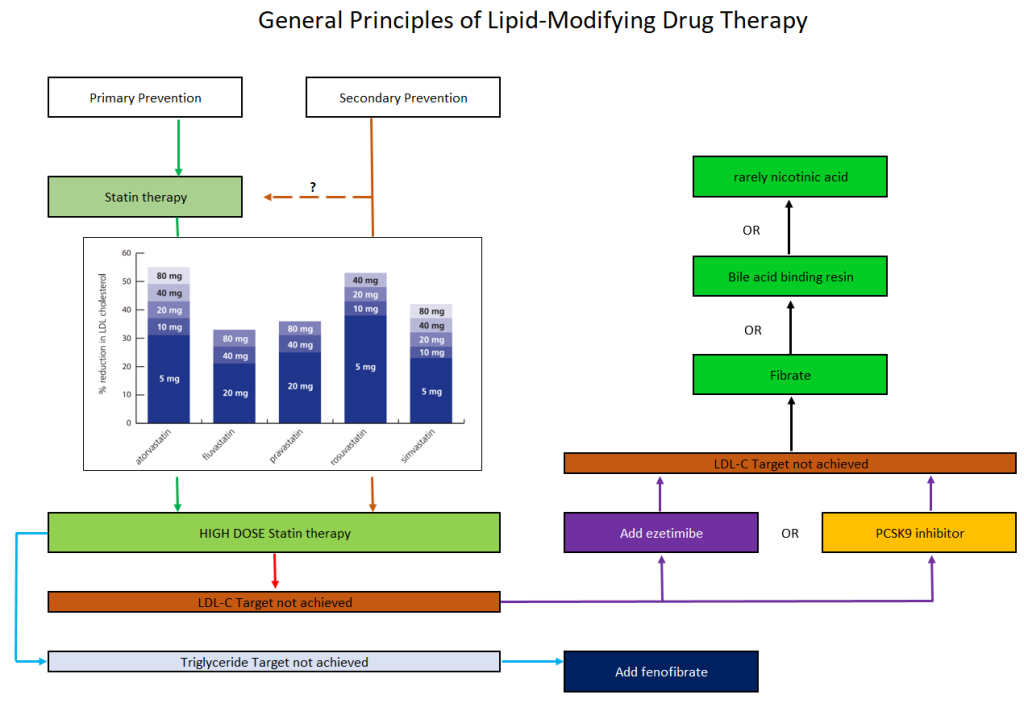
LDL-C Management in Lipid-Modifying Therapy – Pharmacotherapy
LDL-C (low-density lipoprotein cholesterol) is the primary target of lipid-modifying therapy due to its strong relationship with cardiovascular events. There is a continuous correlation between the extent of LDL-C reduction and the decrease in cardiovascular events, making it crucial to lower LDL-C levels. Although achieving target lipid levels can be challenging, any progress towards the target is beneficial. Statins are typically the first-line treatment in addition to non-drug therapies, such as lifestyle changes. Potent statins like atorvastatin or rosuvastatin are commonly used. A low to mid-range dose of a statin can be initiated. For patients assessed at high risk or higher for cardiovascular disease (CVD), a high dose of a potent statin may be started.
The effect of the statin is evaluated after six weeks. If the target range is not achieved, ezetimibe or a PCSK9 inhibitor can be added. Ezetimibe is typically the next choice due to its efficacy and cost-effectiveness. If triglyceride levels are not within the target range, adding a fibrate may be considered.
📺 Watch video: Approach to drug management – hyperlipidaemia. (6:54 min)
Introduction to Other Drugs Used to Manage Dyslipideamia
Bile acid binding resins bind to bile in the small intestine reducing its reabsorption. This increases the clearance of cholesterol and reduces recirculation of bile acids. Because less bile is being reabsorbed, the liver scavenges cholesterol from the plasma to make more bile. This lowers serum cholesterol levels. Bile acid binding resins can reduce LDL-C by 15-25% but may also increase triglycerides. The mechanism of action of the bile acid binding resins is shown at point E in the figure above.
Nicotinic acid is rarely used and is thought to act by reducing VLDL and LDL production.
Fish oil suppresses hepatic triglyceride and VLDL production. Fish oil is mainly used to treat hypertriglyceridaemia.
📺 Watch video: Pharmacology of less common drugs to lower cholesterol. (5:00 min)
Summary
Hyperlipidemia and dyslipidemia are sometimes used interchangeably but this is technically incorrect. They both indicate a derangement of lipid profile. Dyslipidemia is a broader term accepted to cover elevations in plasma cholesterol
Cholesterol is a major risk factor for CVD and stroke
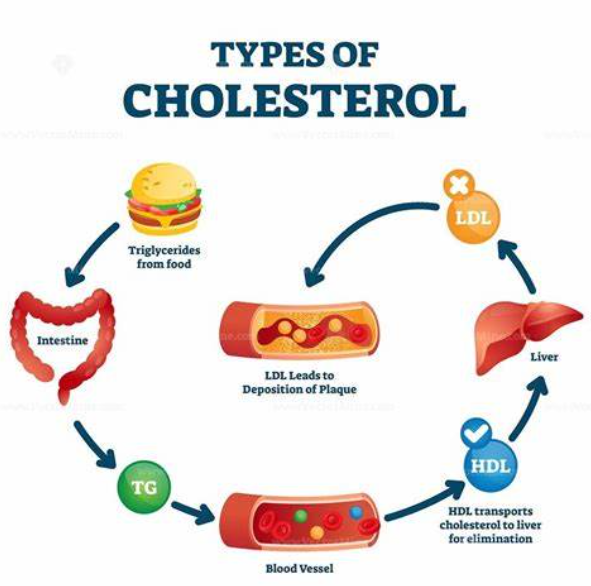
Cholesterol comes from two sources – the exogenous pathway absorbed from diet and the endogenous pathway – cholesterol produced by the liver
There are three major lipids reported in lipid studies – LDL-C which is also known as bad cholesterol. It is responsible for transporting cholesterol to the peripheral tissues. HDL-C which is also known as good cholesterol which is responsible for transporting excess cholesterol from the peripheries to the liver for use or elimination and triglycerides – excess energy typically stored in adipose tissue. It is associated with liver dysfunction and pancreatitis.
Approaches to cholesterol control are dependent on the patient’s risk of developing cardiovascular disease in the next 5 years. The higher the risk, the more aggressive the therapy approach.
Non-drug therapy is critical to lowering elevated cholesterol. It is beneficial also when added to pharmacotherapy.
There are 7 drug classes that reduce cholesterol. The most commonly used 4 classes are the statins (HMG-CoA reductase inhibitors), the fibrates, ezetimibe (a brush border enzyme inhibitor) and the PSCK-9 inhibitors.
COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING
This material has been reproduced and communicated to you by or on behalf of James Cook University in accordance with section 113P of the Copyright Act 1969 (Act).
The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice.