4.1.2 Management of Heart Failure (with Reduced Ejection Fraction)
Management of Heart Failure with Reduced Ejection Fraction (HFrEF)
 |
 |
 |
- Relieve symptoms
- Improve quality of life
- Slow disease progression
- Prevent acute exacerbations / hospitalisation
- Prolong active life.
Non-pharmacological and pharmacological measures are used to achieve these aims. Expand the accordion below to read an overview of the management of HFrEF.
🎞️ Video 1: Aims of Treatment and Overall Management of HFrEF⏲️21:06 mins
Non-Pharmacological Management
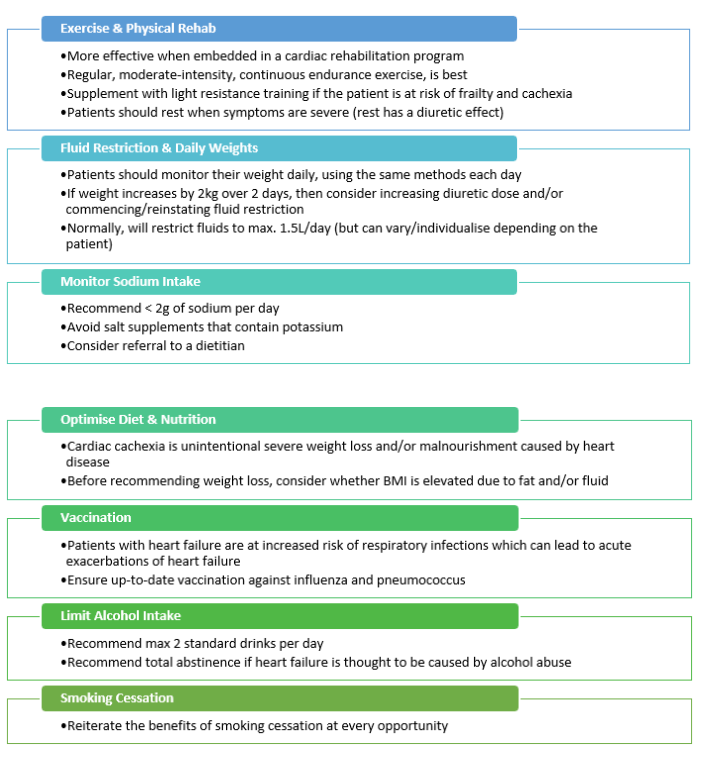
Non-pharmacological treatment strategies are an essential consideration. These are as important as pharmacological treatment for heart failure.
Pharmacological Management
- Angiotensin-Converting Enzyme (ACE) inhibitors or Angiotensin-Receptor Blockers (ARBs) or Angiotensin-Receptor Neprilysin Inhibitors (ARNI) *
- Aldosterone antagonists
- Beta-blockers (HF-specific)
- Sodium-glucose cotransporter 2 (SGLT2) inhibitors
Patients with HFrEF should be prescribed one medication from each of the 4 pillars outlined below, for mortality benefits, unless contraindicated or not tolerated.
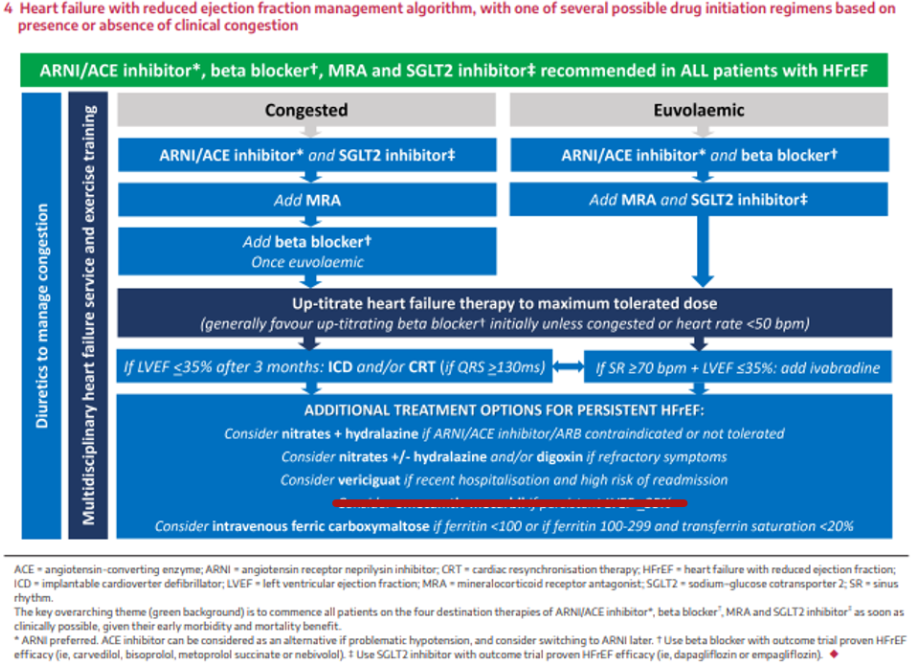 From this image you can see:
From this image you can see:
- The management of HfrEF is divided down the middle. It is split depending on whether the patient presents with overt signs and symptoms congestion or without any signs and symptoms of congestion (in which case they would be considered euvolaemic or ‘not fluid overloaded’). The main difference between the 2 is that beta blockers aren’t started if the patient is congested at the time of their diagnosis (beta blockers aren’t started until the patient is euvolaemic).
- A strong recommendation for use of the 4 pillars at the top of this figure in the green box.
- An upwards titration the doses of the 4 pillar heart failure therapies according to tolerability.
- Diuretics on the left spanning vertically across every row alongside the non-pharmacological recommendations. So, diuretics can be used whenever needed to help to manage congestion, on top of other maintenance therapies outlined in this figure.
- Additional or treatment options for persistent HFrEF.
As a general rule, doses of all agents used for heart failure are started at a low dose and gradually titrated upwards (~ every 2-4 weeks) according to tolerability to the maximum recommended dose. If adverse effects (e.g., low blood pressure, declining renal function, or rising potassium) are problematic, then is better to have low doses of most/all of the pillars than it is to have a high dose of only one pillar.
With regards to duration of drug therapy in HFrEF, the current recommendation is for neurohormonal antagonists (ACEI/ARB/or ARNI, and MRA, and beta blocker) to be continued long-term at target doses even if the ejection fraction recovers, unless the reversible cause of the heart failure has been identified and corrected.
🎞️ Video 2: Pharmacological Management of HFrEF⏲️21:06 mins
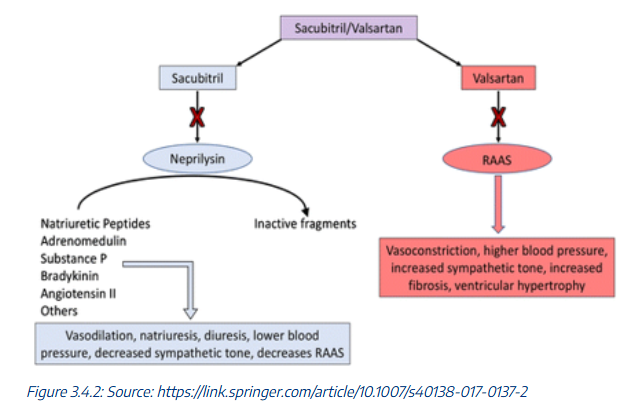
Angiotensin Receptor Neprilysin Inhibitor (ARNI)
The only available ARNI is a combination of sacubitril + valsartan. Sacubitril is a drug that works to increase circulating concentrations of natriuretic peptides. Valsartan is needed to block angiotensin II, because angiotensin II concentrations are increased by sacubitril. Valsartan also works synergistically with sacubitril to decrease activity of the RAAS.
According to current consensus guidelines, an ARNI may be started first line, without the need to transition from an ACEI or ARB. However, this is not often seen in practice, because of current PBS restrictions and the private cost to the patient. At the time of writing, sacubitril + valsartan (Entresto®) is only PBS-subsidised as a second-line agent. It is only subsided if a patient remained symptomatic despite an ACEI or ARB and a beta blocker for a period. In practice, therapy is escalated to an ARNI if the patient has persistently reduced ejection fraction < 40% despite having been on an ACEI or ARB plus a beta blocker for 3-6 months at the maximum tolerated maintenance dose of these medications.
The ARNI should never be used with:
- An ACEI
If an ARNI is initiated, the original ACEI or ARB must be discontinued first. Furthermore, there must be a 36-hour washout period between the last dose of the ACEI and the first dose of the ARNI. An ARNI and ACEI cannot be used together.
The ARNI should be used with:
- A MRA (aldosterone antagonist), AND
- A heart failure – specific beta blocker, AND
- A SGLT2i and a beta blocker) for additional mortality benefits.
Contraindications, precautions, and adverse effects of sacubitril+valsartan are similar ACEIs. Use the accordion below to explore these topics further.
Sodium-Glucose Co-Transporter 2 Inhibitors (SGLT2 Inhibitors)
The pharmacology of SGLT2 inhibitors is discussed later with the diabetes content. However, the cardiovascular benefits of SGLT2 inhibitors are thought to be a result of their haemodynamic and metabolic effects. This is demonstrated in the figure below:
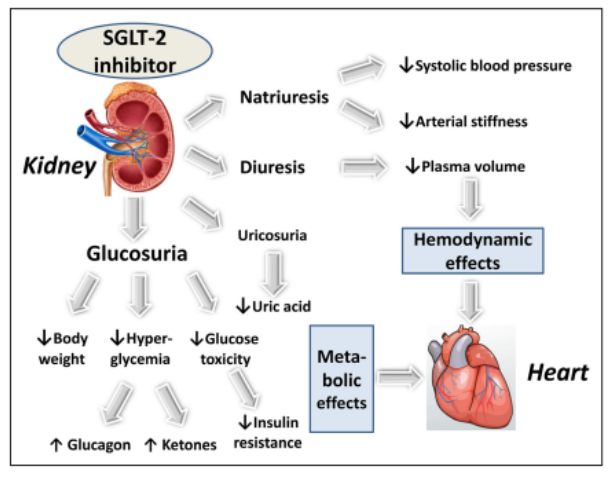 Source: Scheen A. Cardiovascular effects of new oral glucose-lowering agents. Circulation Research. 2018; 122:1439-1459
Source: Scheen A. Cardiovascular effects of new oral glucose-lowering agents. Circulation Research. 2018; 122:1439-1459
Diuretics
Diuretics are indicated to manage clinical signs and symptoms associated with heart failure.
There are no proven mortality benefits associated with the use of diuretics. However, they are still an essential consideration, because they do help patients prevent and treat congestion due to heart failure, and improve quality of life. Sometimes, patients will be prescribed diuretics to take the same dose each day. Other times, patients might just need a dose every now and then (in which case PRN use is also appropriate).
- Loop diuretics are better than thiazide diuretics in the context of heart failure management because they cause more free water clearance by the kidneys and have a faster onset of action too. Examples of loop diuretics include furosemide and bumetanide.
Refer to week 2 content (chapter 2.1.4) to revise the pharmacology of diuretics.
Download the lecture notes here:
COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING
This material has been reproduced and communicated to you by or on behalf of James Cook University in accordance with section 113P of the Copyright Act 1969 (Act).
The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice.