8.3 Asthma
Learning Outcomes
Be able to:
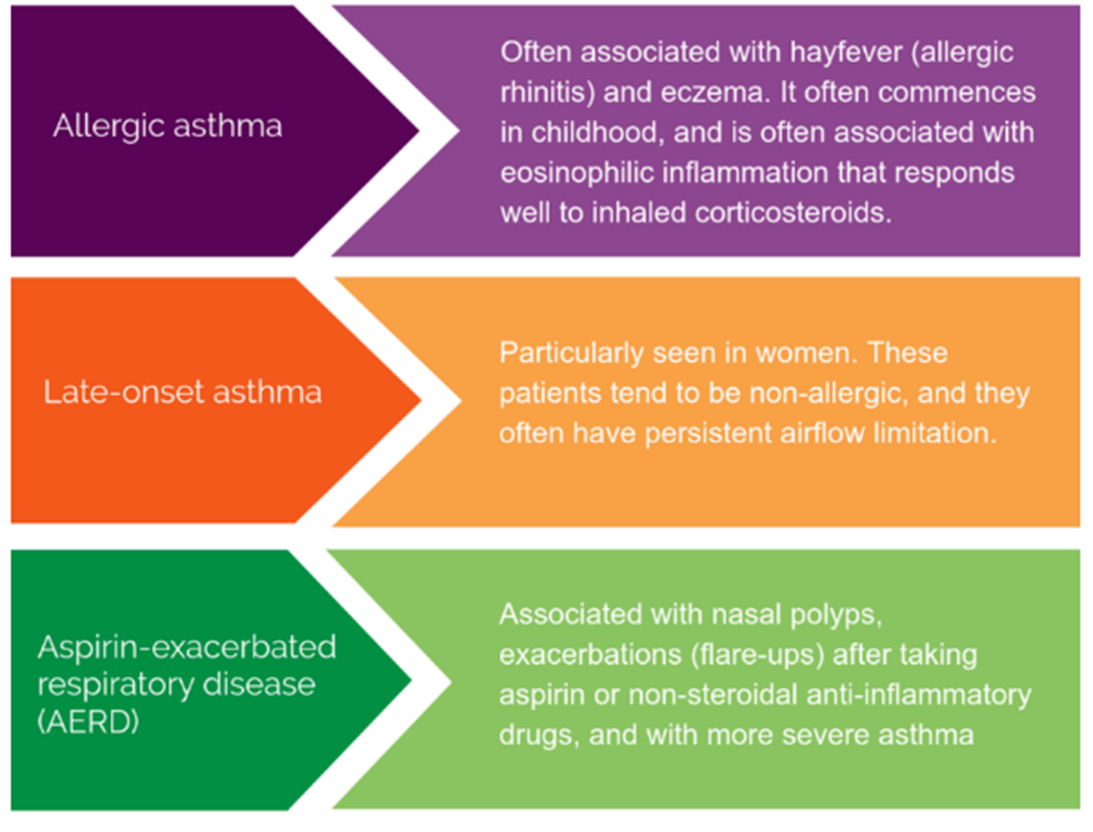
- Explain the pathophysiology and clinical presentation of asthma
- Describe the prevalence of asthma and its impact on the Australian population
- Differentiate between the different forms of asthma
- Recognise the risk factors for asthma
- Relate the diagnostic criteria and investigations to new presentations and ongoing asthma control
- Relate the mechanism of action of medications commonly used to the treatment of asthma
- Provide basic advice and clinical management for presentations of asthma.
Asthma Resources
There are some very useful clinical asthma resources worth reviewing. I recommend you look at the Australian Asthma Handbook developed by the National Asthma Council. It is available from https://www.asthmahandbook.org.au/. You should also familiarise yourself with eTherapeutic Guidelines available through the JCU library database.
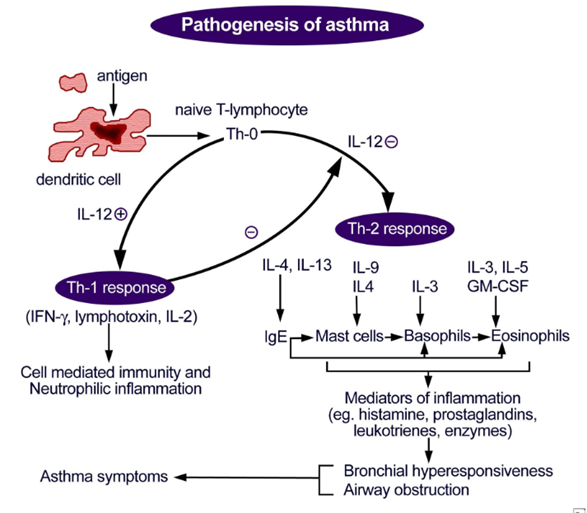
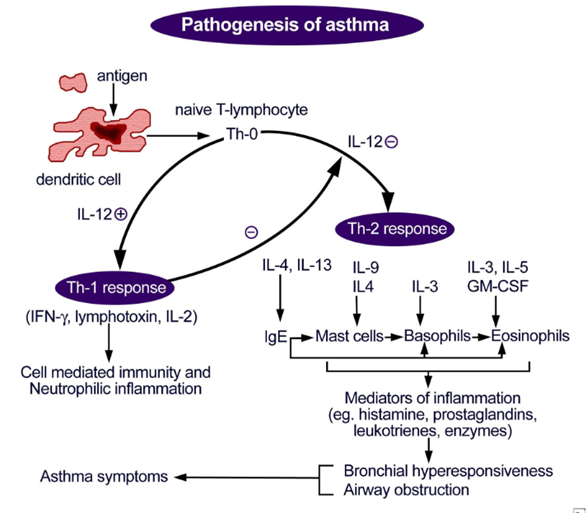
Pathophysiology
Asthma is a chronic, inflammatory disorder of the airways involving reversible airway obstruction. Asthma occurs due to inappropriate inflammation and hyperresponsiveness to triggers. These stimuli may include any of the following:
- Environmental triggers (e.g., smoke, allergens, cold or dry air, perfumes)
- Pharmacological triggers (e.g., NSAIDs, aspirin, beta blockers and cholinergic agents)
- Exercise
- Physiological and psychological changes (e.g. extreme emotions, hormonal changes, pregnancy and sexual activity)
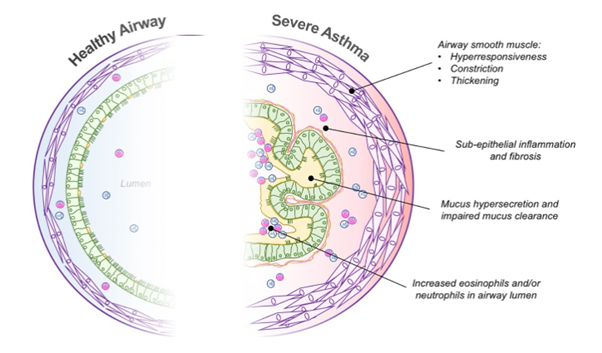
In response to these stimuli, a range of inflammatory mediators are released. The release of eosinophils, leukotrienes and leucocytes cause bronchoconstriction of airway smooth muscle, bronchiole oedema and mucous production, which narrows the airway and limits the passage of air to alveoli for gas exchange. Additionally, these inflammatory mediators also produce a sub-acute inflammatory response leading to permanent airway remodeling. Permanent airway remodeling can involve increased collagen deposition, thickening of basement membrane and increase in expression of goblet cells.
Symptoms of airway obstruction associated with asthma include:
- Cough
- Wheeze
- Breathlessness
- Chest discomfort or tightness
- Increased respiratory rate and work of breathing (in children)
Asthma is linked to a history of atopic disorder (allergic rhinitis or atopic dermatitis) and a family history of asthma or atopic disorder.
There are 3 different phenotypes of asthma. These include allergic asthma, late-onset asthma and aspirin-exacerbated respiratory disease (AERD).
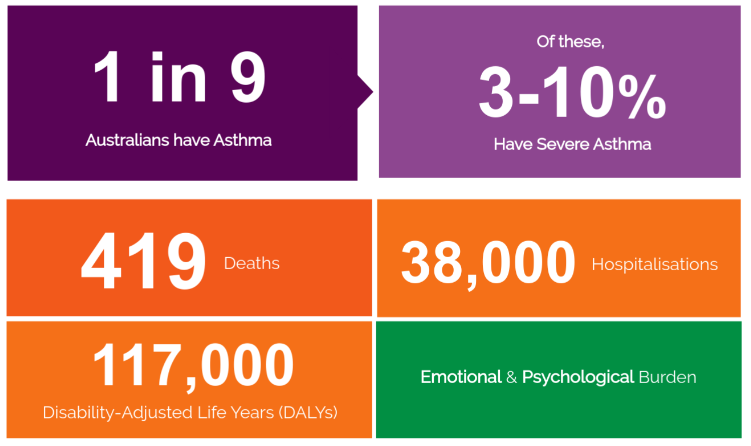
Epidemiology
Asthma is a common chronic condition in children, with about 1 in 10 boys and 1 in 16 girls under 15 years having asthma. Asthma has a major impact on individuals, their carers and Australia’s health system. In 2022-2023 there were over 31,000 hospitalisations where asthma was the main diagnosis. Almost half (43%) of these were for children aged 14 or under. Over 90% of asthma hospitalisations were considered potentially avoidable with optimised care in the community. People with asthma are more likely to report a poor quality of life, especially those with severe or poorly controlled asthma. In 2020-21, asthma directly cost the health system $852 million for services provided through general practice, hospitals, government funded medicines, dental services and referrals to specialists and testing. A recent study estimated that poorly controlled asthma costs the healthcare system about $4,600 per person per year. There were 474 deaths due to asthma in 2023.
Diagnosis of Asthma In Adults, Adolescents and Children > 6 years
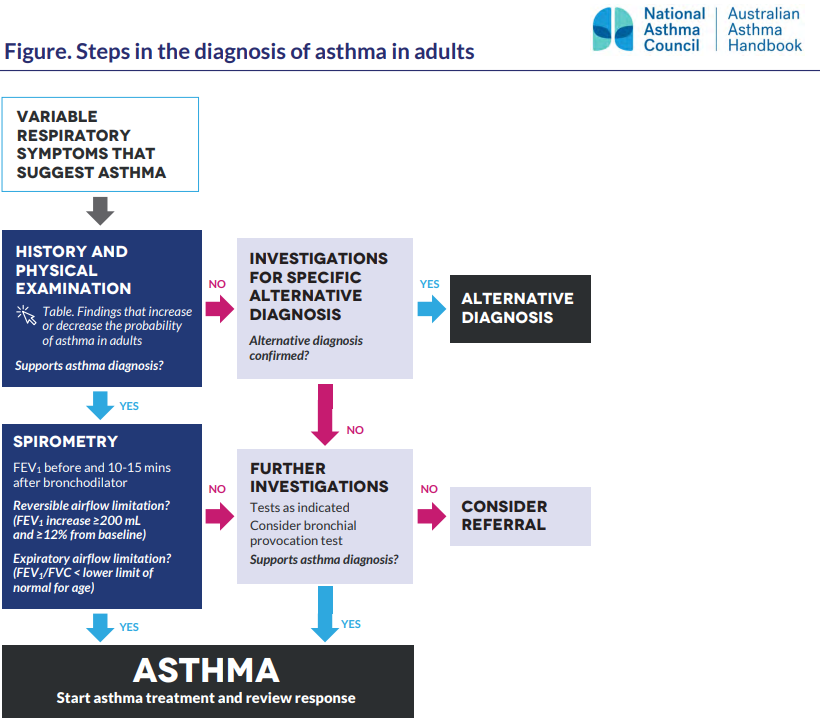
The diagnosis of asthma in adults, adolescents and school-aged children is based on clinical assessment supported by lung function tests. Firstly, a clinical history and examination can determine the likely probability that symptoms (such as cough, chest tightness, wheeze and shortness of breath) and clinical findings are due to asthma. Then, confirmation of the diagnosis can occur via lung function tests that are used at a time when the patient does not have a respiratory tract infection. Spirometry is key to confirm a diagnosis of asthma. It should be arranged and performed for every adult patient, adolescent and child > 6 years with suspected asthma. You should remember from the previous chapter that spirometry is used to measure FEV1 and FVC and can be performed before and after administration of a bronchodilator, such as salbutamol via a spacer.
Spirometry findings that would support a diagnosis of asthma in adults and adolescents include:
- Expiratory airflow limitation demonstrated by FEV1/FVC ratio less than lower limit of normal for age
- Expiratory airflow limitation that is reversible (variable) demonstrated by an increase in FEV1 of at least 200 mL and 12% from baseline 10 to 15 minutes after giving a short-acting beta2 agonist. A larger increase in FEV1 (eg more than 400 mL) in response to a SABA is strongly supportive of asthma.
In school-aged children (6-11 years) who are able to perform spirometry, the diagnosis of asthma is supported by finding of:
- Expiratory airflow limitation that is reversible (variable) demonstrated by FEV1 increase ≥12% from baseline post bronchodilator.
Patients with asthma typically show significant reversibility of the obstructive symptoms of asthma (i.e. variation in expiratory airflow that is greater than that seen in healthy patients). In the diagram below, you can see that there is in improvement in FVC and FEV1 after exposure to a bronchodilator (salbutamol = green line). The evidence for variable airflow limitation must be documented at the time of asthma diagnosis in adults, adolescents and children > 6 years.
Look at the “Steps in the diagnosis of asthma in adults” from the National Asthma Handbook. It is also available here: Figure_Steps-in-the-diagnosis-of-asthma-in-adults_web.
Then, look at the “Steps in the diagnosis of asthma in children aged 6 years and over”. It is also available here: Figure_Steps-in-the-diagnosis-of-asthma-in-children-aged-6-years-and-over_web_LR
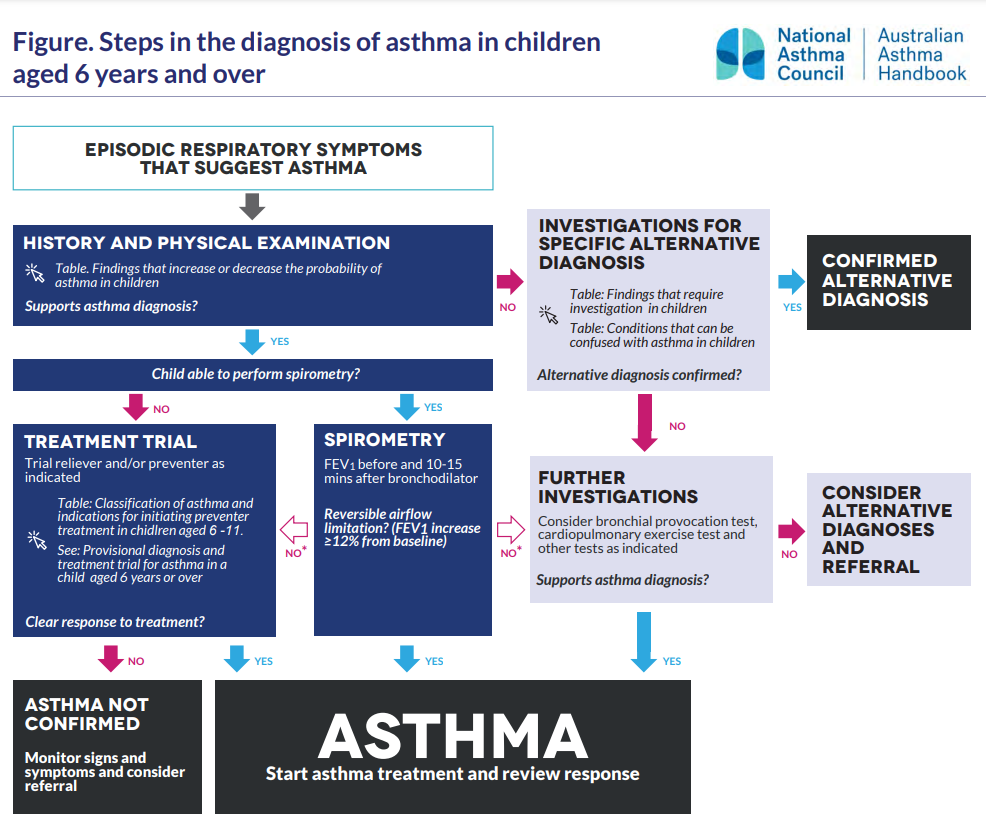
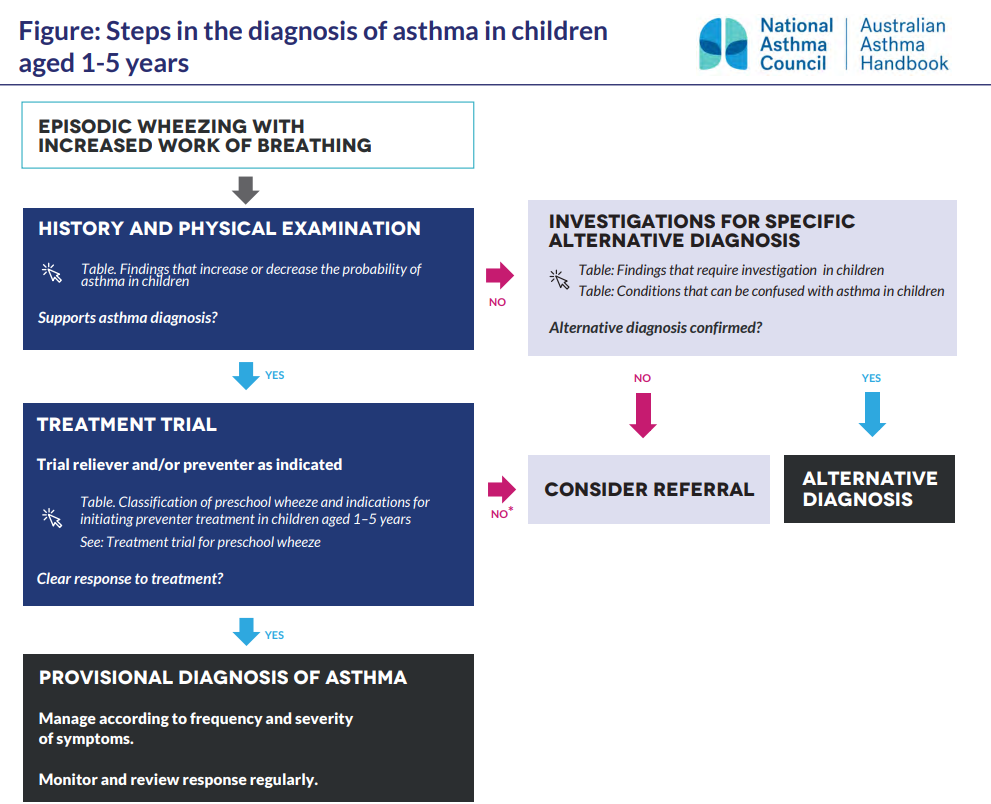
Diagnosis of Asthma In Children < 6 years
Asthma should not be diagnosed in infants aged less than 12 months. Wheezing in infants younger than 12 months is most commonly a symptom of acute viral bronchiolitis rather than asthma. In young children aged 1-5 years years it is difficult to make the diagnosis of asthma with a high degree of certainty because:
Laboratory Test and Imaging
No pathology tests are routinely recommended during the assessment and management of non-severe asthma in adults. It is important to note that some comorbidities and rarely used therapies (e.g., theophylline) may require monitoring. Assessment of allergy status, inflammatory markers, sputum and/or peripheral blood eosinophil count and exhaled nitric oxide tests may be performed by a medical practitioner. This is especially important in the management of severe asthma and assessment of eligibility for therapies such as monoclonal antibody therapies (e.g., benralizumab) under the guidance of a respiratory specialist. A chest X-ray is not necessary for diagnosis of asthma.
📺 Watch this video on the introduction to asthma, triggers and diagnosis of asthma (18:17 mins)
Lifestyle Advice for Asthma
The mainstay of non-pharmacological management and lifestyle advice for asthma is the avoidance or management of triggers, adoption of healthy lifestyle, self management and ongoing review. Use the accordion below to find out more.
Pharmacological Management of Asthma In Adults and Adolescents
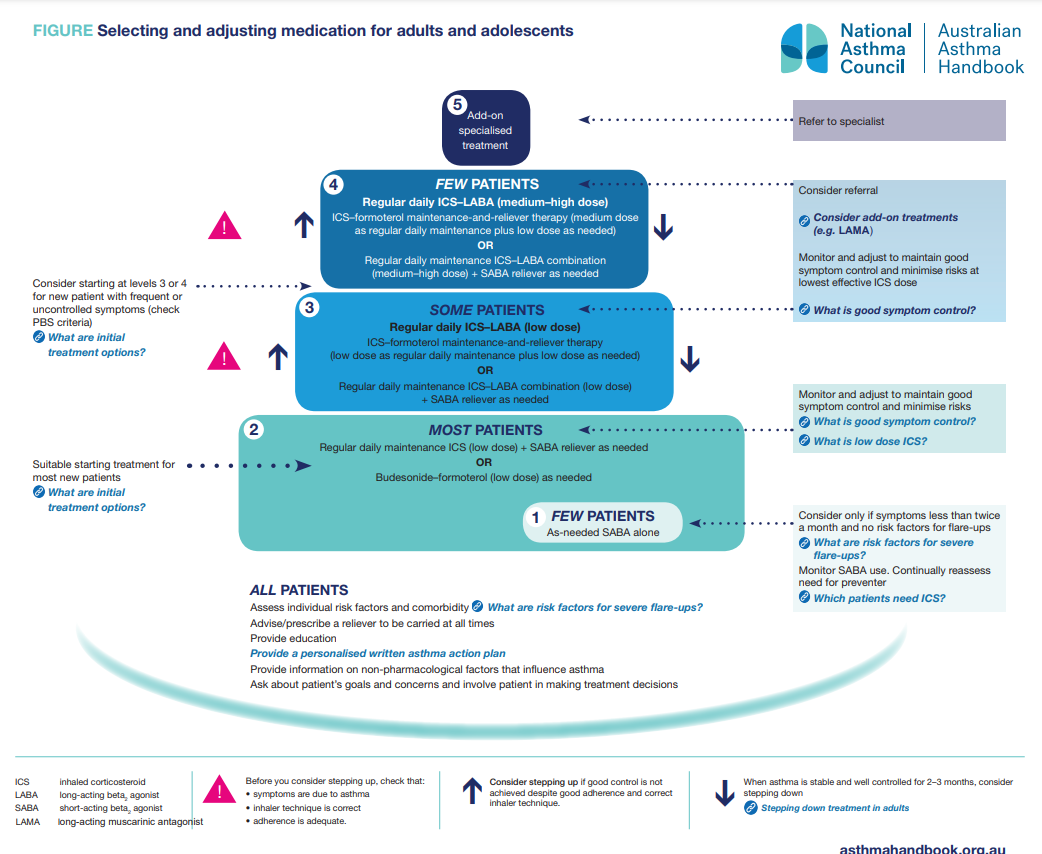
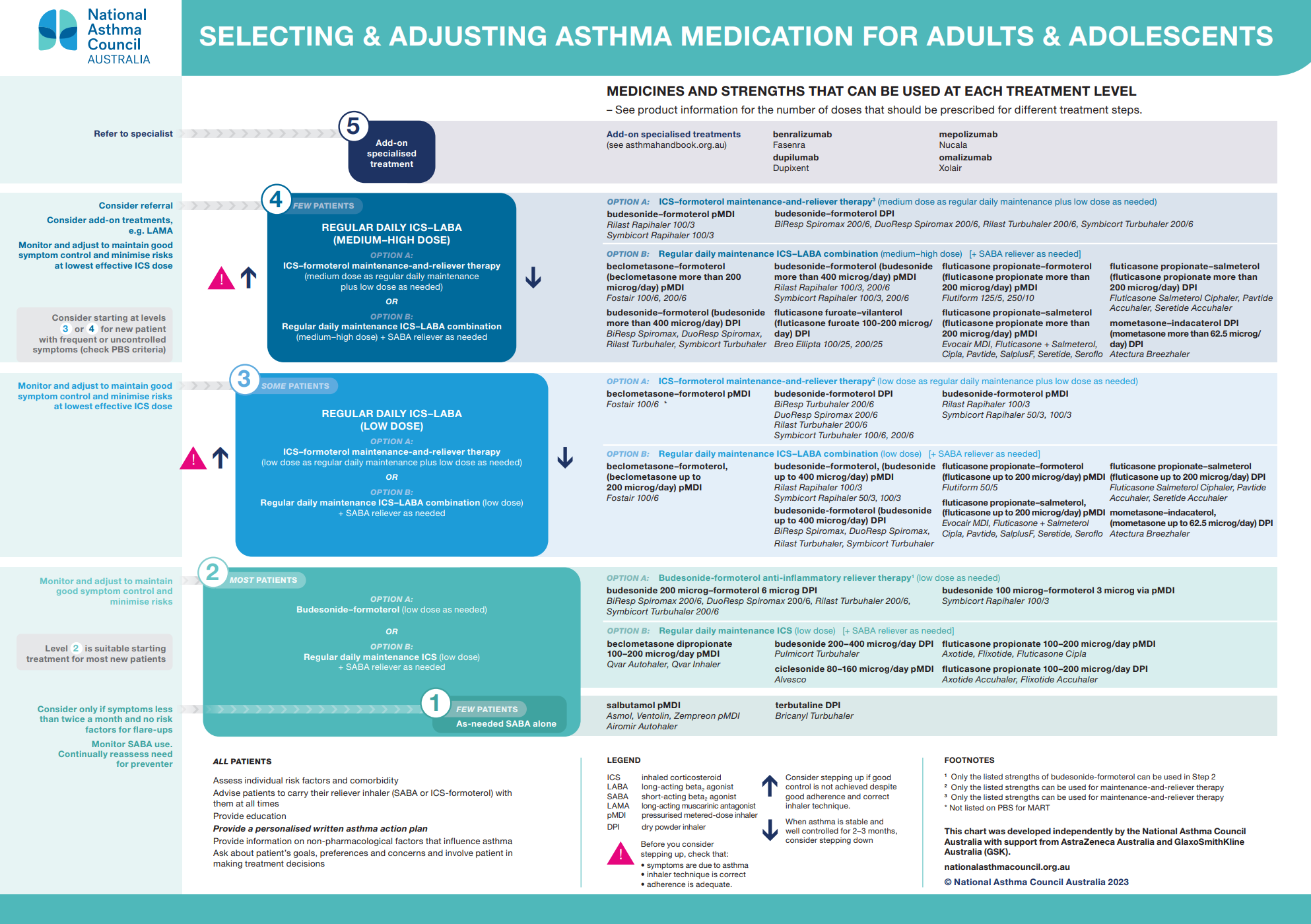
The following accordion may help to understand the diagram above
Stepping Up
The aim of management of asthma in adults and adolescents is to maintain a normal quality of life, free of asthma symptoms and exacerbations, and without adverse effects of asthma treatment. It also aims to prevent long-term lung damage. Drug treatment for asthma in adults and adolescents is introduced in a stepwise manner. Most patients start at Step 2 and initial treatment options include either regular daily low dose ICS + SABA as needed, or, low dose budesonide-formoterol as needed. The patient should be monitored and pharmacotherapy adjusted to maintain good symptom control whilst minismising adverse effects. What is considered “good” symptom control? We discuss this later in the module. If after 4-6 weeks the patient does not have good asthma control and the symptoms are due to asthma, inhaler technique is correct and adherence is adequate, the prescriber can consider stepping up the regimen.
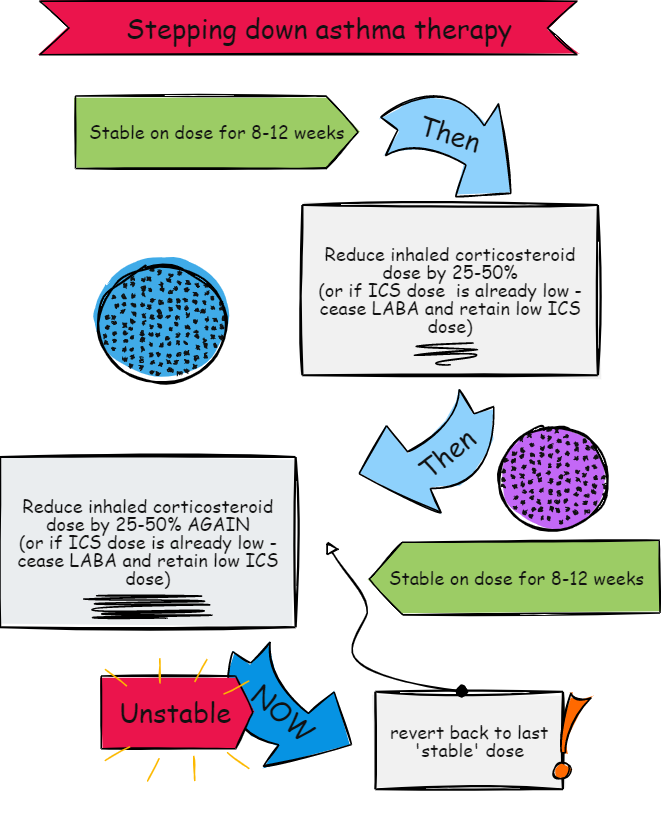
Stepping Down
{kind=link}
📺 Watch this video on asthma management in adults. Please note that the video was created before the National Asthma Council Asthma Handbook was updated so the images of the algorithms look different. The premise of stepping up and stepping down is the same, however. Also note that LRTA (montelukast) is not used in adults anymore and that cromylons are no longer used.
Pharmacological Management of Asthma In Children > 6 years
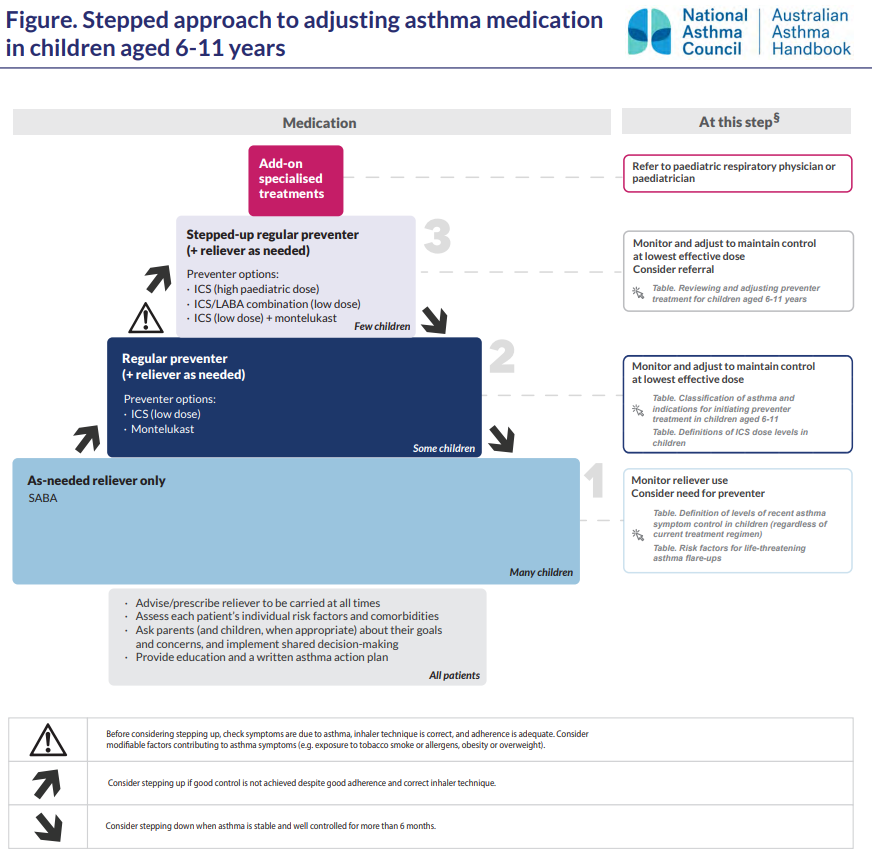
The following accordion may help to understand the diagram above:
Stepping Up
In children aged over 6 years, a diagnosis of asthma can be made with more certainty as school-aged children are likely to be able to perform spirometry. We have already discussed how the presence of reversible (variable) expiratory airflow limitation on spirometry supports the diagnosis of asthma after history and clinical findings increase the likeness of asthma. Most children aged 6-11 years are able to maintain good asthma control with use of a SABA as needed. Some children require preventer treatment with regular daily low dose lCS + SABA as needed or regular daily LTRA + SABA as needed. Indications for initiating preventor treatment in children aged 6-11 years include any of the following:
- Flare-ups every 6 weeks or more often
- Persistent asthma symptoms
- Daytime asthma symptoms > once per week or night-time symptoms > twice per month
- Severe flare-ups, irrespective of the frequency of flare-ups or symptoms between flare-ups
If symptom control is not maintained despite good adherence and inhaler technique, the dose of the ICS may be increased or a combination of regular daily low dose ICS-LABA or regular daily low dose ICS-LTRA + SABA as needed may be added.
Stepping Down
Consider stepping down when asthma is stable and well controlled for more than 6 months.
Pharmacological Management of Asthma In Children < 6 Years
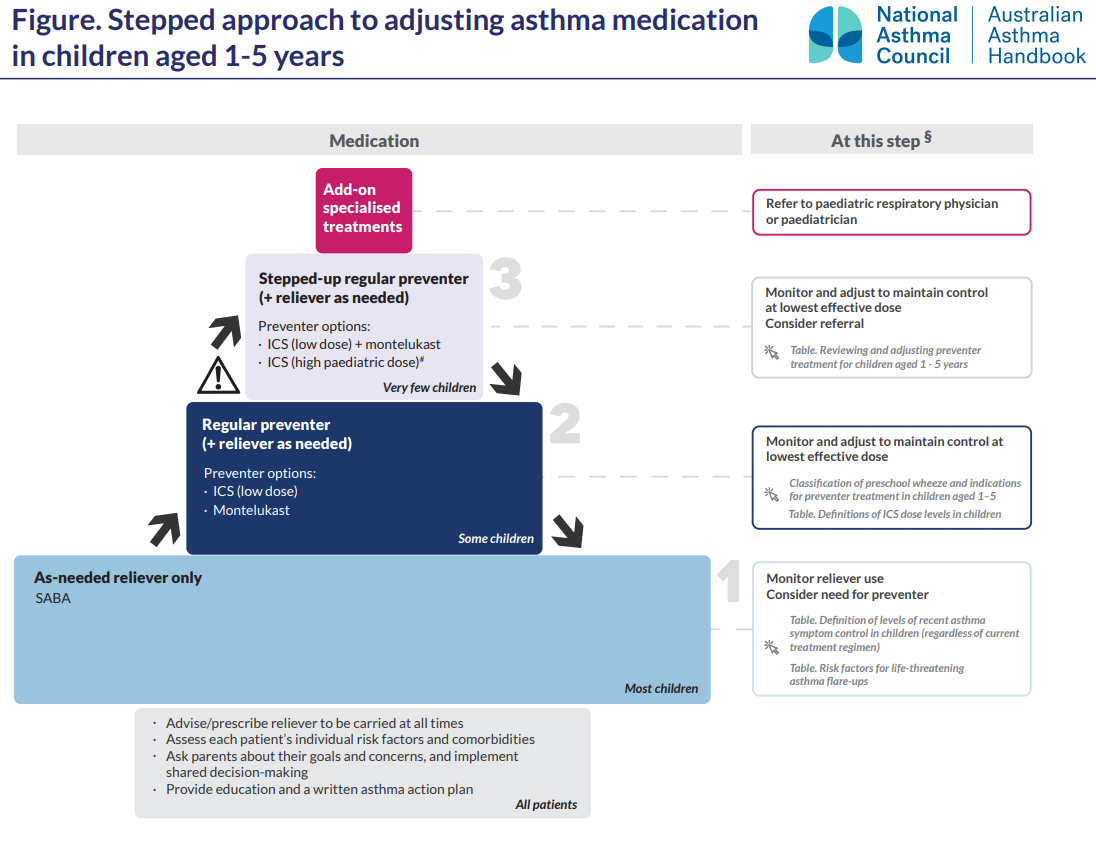
The following accordion may help to understand the diagram above:
Stepping Up
For all children with asthma or salbutamol-responsive preschool wheeze, a reliever and inhaler device suitable for the child’s age is prescribed. Some children aged 2 years and older with frequent symptoms (e.g., wheeze, cough or breathlessness at least once per week) or a history of severe flare-ups (e.g. requiring emergency department visits, intensive care or hospitalisation) may require preventor treatment. A regular daily low dose ICS + SABA as needed or LTRA + SABA as needed can be used to maintain good asthma control. Very few children require regular daily low dose ICS+LTRA + SABA as needed or high paediatric dose ICS + SABA as needed which warrants specialised care.
Stepping Down
Stepping down can be considered by the prescriber when asthma has been well controlled for 6 months. This will help identify the minimal dose or regimen needed to maintain control and may minimise the risk of treatment-related adverse effects and help identify the minimal dose or regimen needed to maintain control.
📺 Watch this video on asthma management in children. Please note that the video was created before the National Asthma Council Asthma Handbook was updated so the images of the algorithms look different. The premise of stepping up and stepping down is the same, however. Also note that cromylons are no longer used.
Asthma Control
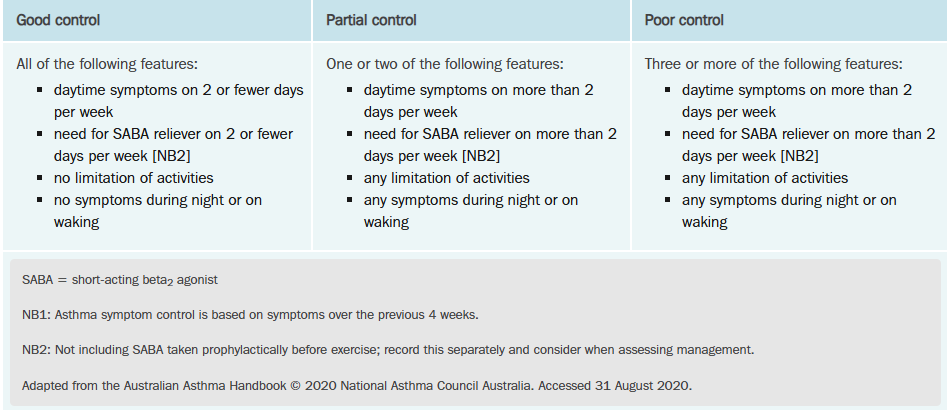
Some risk factors for adverse asthma outcomes include poor adherence, inadequate inhaler technique, poor asthma symptom control, any asthma exacerbation is the previous 12 months, lack of a written asthma management plan and allergic rhinitis and rhinosinusitis. Asthma symptom control should be routinely and opportunistically assessed by pharmacists. Classification of asthma symptom control is based on the frequency of asthma symptoms over the previous 4 weeks, and is classified as good, partial or poor, as detailed in the table below from eTG.
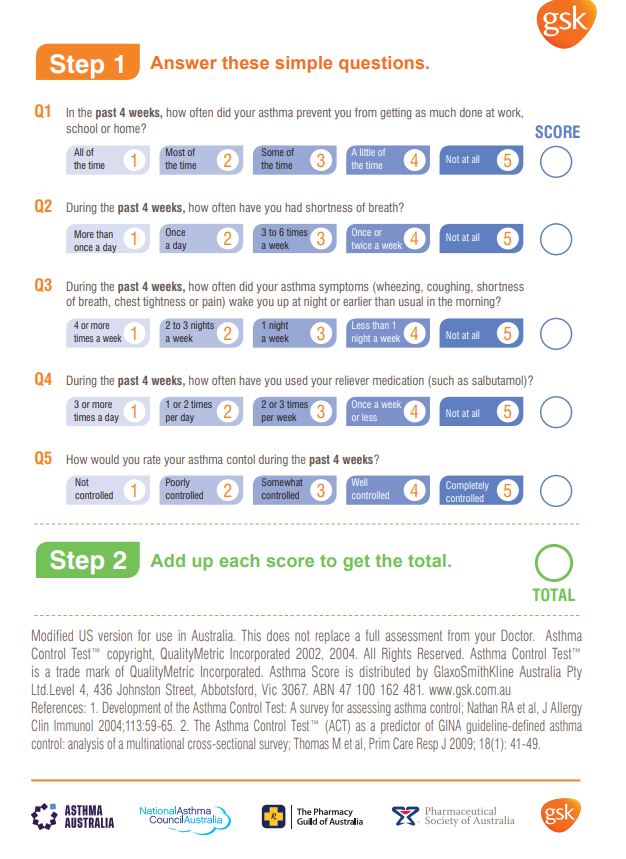
An Asthma Control Test (ACT) can also be used to assess asthma control. ACT score ≥ 20 is good control, ACT score 16 – 19 is partial control and ACT score 5 – 15 is poor control. This tool can be found here: Print-version-ACT-page-2.png (626×859)
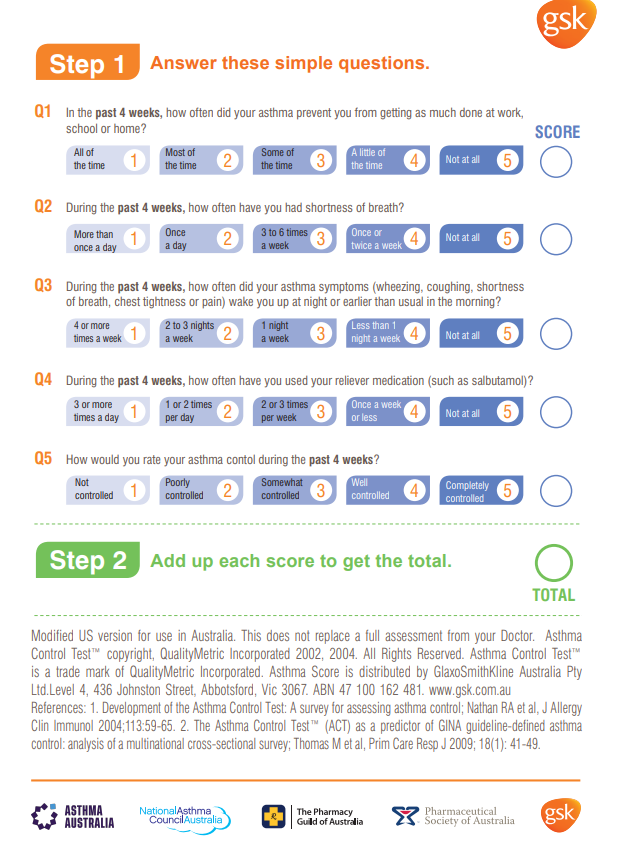{kind=link}
Acute exacerbations, First Aid for Asthma and Written Asthma Management Plans
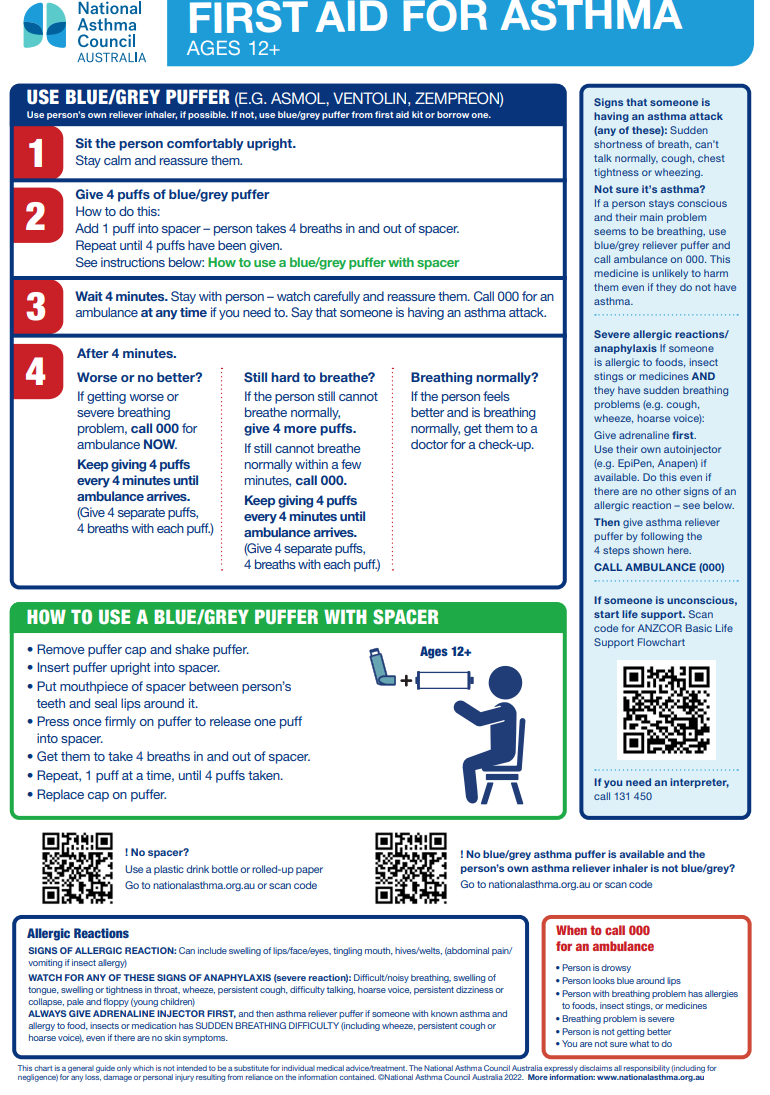
Pharmacists must be able to counsel patients on the signs and symptoms of acute exacerbations, first aid for asthma and the importance written asthma management plans. Use the accordion below to learn more:
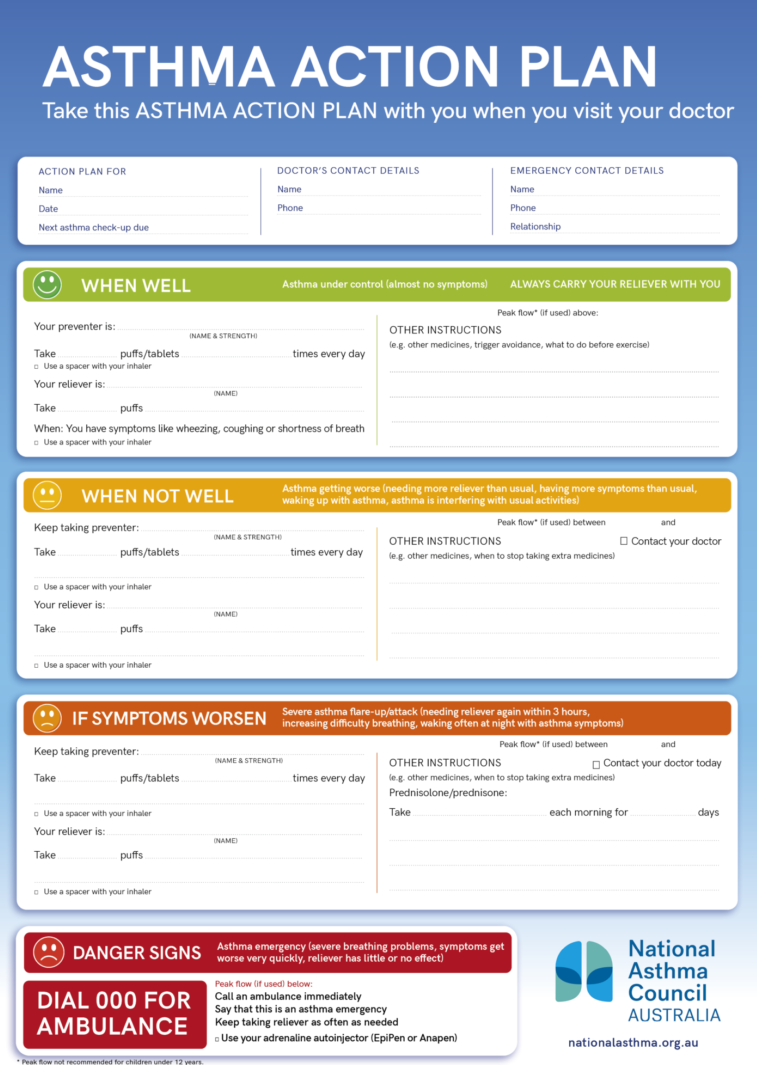
Use these links to preview First Aid for Asthma information sheets:
Symbicort_Asthma_Action_Plan_Rapihaler_01.06.2020
Fostair-Asthma-Action-Plan_Version2
NAC-Asthma-Action-Plan-2023-Update-HD
This material has been reproduced and communicated to you by or on behalf of James Cook University in accordance with section 113P of the Copyright Act 1969 (Act).
The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act. Do not remove this notice.